
Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Hypoglycemia
View on Wikipedia
| Hypoglycemia | |
|---|---|
| Other names | Hypoglycaemia, hypoglycæmia, low blood glucose, low blood sugar |
 | |
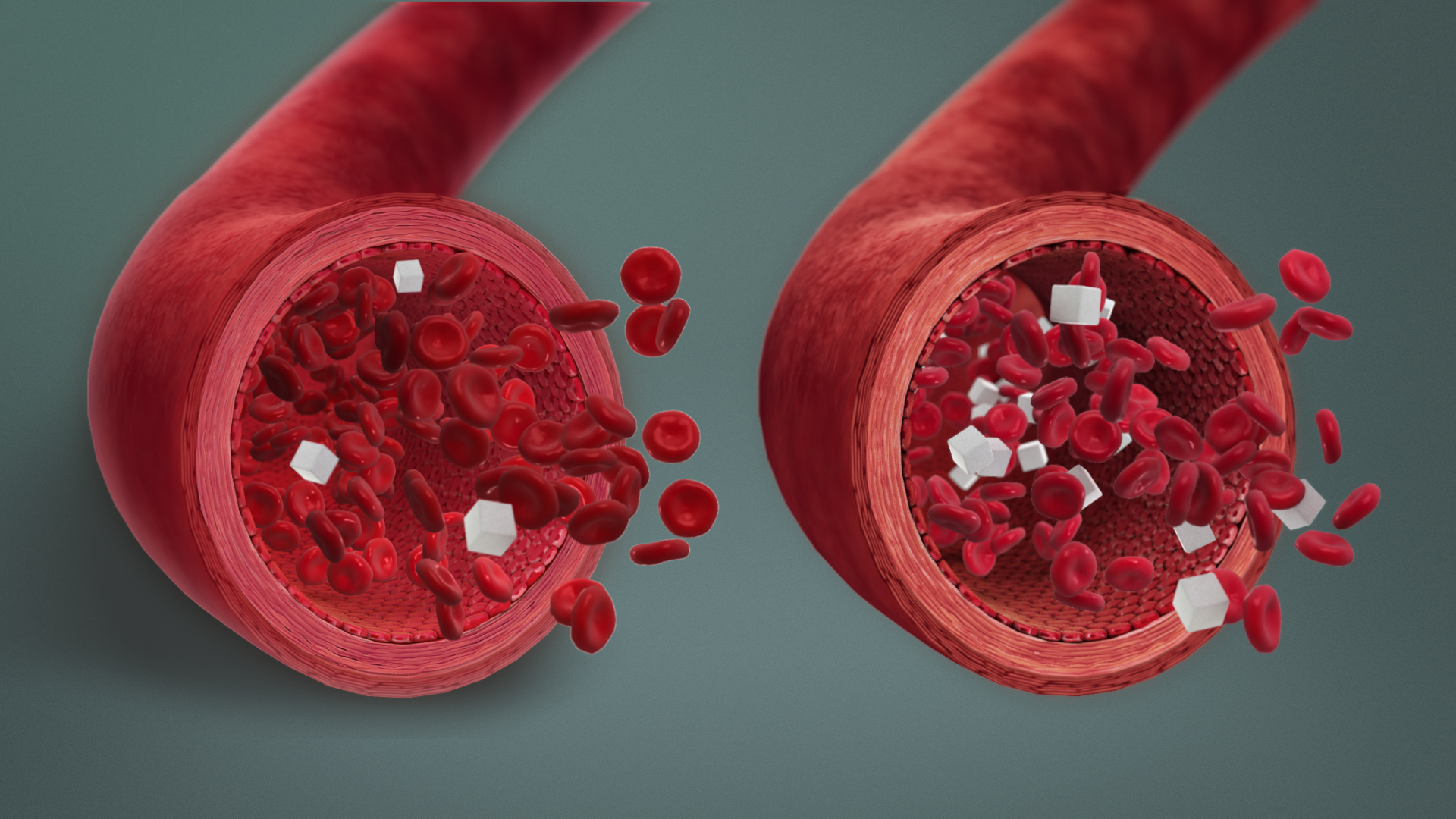
| Hypoglycemia (left) and normal blood sugar concentration (right) | |
| Specialty | Endocrinology |
| Symptoms | Headache, blurred vision, shakiness, dizziness, weakness, fatigue, sweating, clamminess, fast heart rate, anxiety, hunger, nausea, pins and needles sensation, difficulty talking, confusion, unusual behavior, lightheadedness, pale skin color, seizures[1][2][3][4][5] |
| Complications | Loss of consciousness, death, cardiac arrest |
| Usual onset | Rapid[1] |
| Causes | Medications (insulin, glinides, and sulfonylureas), sepsis, kidney failure, certain tumors, liver disease,[1][6] malnutrition[7] |
| Diagnostic method | Whipple's triad: Symptoms of hypoglycemia, serum blood glucose level <70 mg/dL (3.9 mmol/L), and resolution of symptoms when blood glucose returns to normal[2] |
| Treatment | Eating foods high in simple sugars |
| Medication | Glucose, glucagon[1] |
| Frequency | In type 1 diabetics, mild hypoglycemia occurs twice per week on average, and severe hypoglycemia occurs once per year.[3] |
| Deaths | In type 1 diabetics, 6–10% will die of hypoglycemia.[3] |
Hypoglycemia (American English), also spelled hypoglycaemia or hypoglycæmia (British English), sometimes called low blood sugar, is a fall in blood sugar to levels below normal, typically below 70 mg/dL (3.9 mmol/L).[1][3] Whipple's triad is used to properly identify hypoglycemic episodes.[2] It is defined as blood glucose below 70 mg/dL (3.9 mmol/L), symptoms associated with hypoglycemia, and resolution of symptoms when blood sugar returns to normal.[1] Hypoglycemia may result in headache, tiredness, clumsiness, trouble talking, confusion, fast heart rate, sweating, shakiness, nervousness, hunger, loss of consciousness, seizures, or death.[1][3][2] Symptoms typically come on quickly.[1] Symptoms can remain even soon after raised blood level.
The most common cause of hypoglycemia is medications used to treat diabetes such as insulin, sulfonylureas, and biguanides.[3][2][6] Risk is greater in diabetics who have eaten less than usual, recently exercised, or consumed alcohol.[1][3][2] Other causes of hypoglycemia include severe illness, sepsis, kidney failure, liver disease, hormone deficiency, tumors such as insulinomas or non-B cell tumors, inborn errors of metabolism, and several medications.[1][2][3] Low blood sugar may occur in otherwise healthy newborns who have not eaten for a few hours.[8]
Hypoglycemia is treated by eating a sugary food or drink, for example glucose tablets or gel, apple juice, soft drink, or lollipops.[1][3][2] The person must be conscious and able to swallow.[1][3] The goal is to consume 10–20 grams of a carbohydrate to raise blood glucose levels to a minimum of 70 mg/dL (3.9 mmol/L).[3][2] If a person is not able to take food by mouth, glucagon by injection or insufflation may help.[1][3][9] The treatment of hypoglycemia unrelated to diabetes includes treating the underlying problem.[3][2]
Among people with diabetes, prevention starts with learning the signs and symptoms of hypoglycemia.[3][2] Diabetes medications, like insulin, sulfonylureas, and biguanides can also be adjusted or stopped to prevent hypoglycemia.[3][2] Frequent and routine blood glucose testing is recommended.[1][3] Some may find continuous glucose monitors with insulin pumps to be helpful in the management of diabetes and prevention of hypoglycemia.[3]
Definition
[edit]Hypoglycemia, also called low blood sugar or low blood glucose, is a blood-sugar level below 70 mg/dL (3.9 mmol/L).[3][5]
Blood-sugar levels naturally fluctuate throughout the day, the body normally maintaining levels between 70 and 110 mg/dL (3.9–6.1 mmol/L).[3][2] Although 70 mg/dL (3.9 mmol/L) is the lower limit of normal glucose, symptoms of hypoglycemia usually do not occur until blood sugar has fallen to 55 mg/dL (3.0 mmol/L) or lower.[3][2] The blood-glucose level at which symptoms of hypoglycemia develop in someone with several prior episodes of hypoglycemia may be even lower.[2]
Whipple's triad
[edit]The symptoms of low blood sugar alone are not specific enough to characterize a hypoglycemic episode.[2] A single blood sugar reading below 70 mg/dL is also not specific enough to characterize a hypoglycemic episode.[2] Whipple's triad is a set of three conditions that need to be met to accurately characterize a hypoglycemic episode.[2]
The three conditions are the following:
- The signs and symptoms of hypoglycemia are present (see section below on Signs and Symptoms)[2][10]
- A low blood glucose measurement is present, typically less than 70 mg/dL (3.9 mmol/L)[2]
- The signs and symptoms of hypoglycemia resolve after blood glucose levels have returned to normal[2]
Age
[edit]The biggest difference in blood glucose levels between the adult and pediatric population occurs in newborns during the first 48 hours of life.[8] After the first 48 hours of life, the Pediatric Endocrine Society cites that there is little difference in blood glucose level and the use of glucose between adults and children.[8] During the 48-hour neonatal period, the neonate adjusts glucagon and epinephrine levels following birth, which may cause temporary hypoglycemia.[8] As a result, there has been difficulty in developing guidelines on interpretation and treatment of low blood glucose in neonates aged less than 48 hours.[8] Following a data review, the Pediatric Endocrine Society concluded that neonates aged less than 48 hours begin to respond to hypoglycemia at serum glucose levels of 55–65 mg/dL (3.0–3.6 mmol/L).[8] This is contrasted by the value in adults, children, and older infants, which is approximately 80–85 mg/dL (4.4–4.7 mmol/L).[8]
In children who are aged greater than 48 hours, serum glucose on average ranges from 70 to 100 mg/dL (3.9–5.5 mmol/L), similar to adults.[8] Elderly patients and patients who take diabetes pills such as sulfonylureas are more likely to suffer from a severe hypoglycemic episode.[11][12] Whipple's triad is used to identify hypoglycemia in children who can communicate their symptoms.[8]
Signs and symptoms
[edit]Hypoglycemic symptoms are divided into two main categories.[3] The first category is symptoms caused by low glucose in the brain, called neuroglycopenic symptoms.[3] The second category of symptoms is caused by the body's reaction to low glucose in the blood, called adrenergic symptoms.[3]
| Neuroglycopenic symptoms | Adrenergic symptoms |
|---|---|
|
|
| References:[1][3][2][5][4][13][medical citation needed][14][medical citation needed] | |
Everyone experiences different symptoms of hypoglycemia, so someone with hypoglycemia may not have all of the symptoms listed above.[3][5][4] Symptoms also tend to have quick onset.[5] It is important to quickly obtain a blood glucose measurement in someone presenting with symptoms of hypoglycemia to properly identify the hypoglycemic episode.[5][2]
Causes
[edit]Hypoglycemia is most common in those with diabetes treated by insulin, glinides, and sulfonylureas.[3][2] Hypoglycemia is rare in those without diabetes, because there are many regulatory mechanisms in place to appropriately balance glucose, insulin, and glucagon.[3][2]
Diabetics
[edit]Medications
[edit]The most common cause of hypoglycemia in diabetics is medications used to treat diabetes such as insulin, sulfonylureas, and biguanides.[3][2][6] This is often due to excessive doses or poorly timed doses.[3] Sometimes diabetics may take insulin in anticipation of a meal or snack; then forgetting or missing eating that meal or snack can lead to hypoglycemia.[3] This is due to increased insulin without the presence of glucose from the planned meal.[3]
Hypoglycemic unawareness
[edit]Recurrent episodes of hypoglycemia can lead to hypoglycemic unawareness, or the decreased ability to recognize hypoglycemia.[15][16][17] As diabetics experience more episodes of hypoglycemia, the blood glucose level which triggers symptoms of hypoglycemia decreases.[15][16][17] In other words, people without hypoglycemic unawareness experience symptoms of hypoglycemia at a blood glucose of about 55 mg/dL (3.0 mmol/L).[3][2] Those with hypoglycemic unawareness experience the symptoms of hypoglycemia at far lower levels of blood glucose.[15][16][17] This is dangerous for a number of reasons.[15][16][17] The hypoglycemic person not only gains awareness of hypoglycemia at very low blood glucose levels, but they also require high levels of carbohydrates or glucagon to recover their blood glucose to normal levels.[15][16][17] These individuals are also at far greater risk of severe hypoglycemia.[15][16][17]
While the exact cause of hypoglycemic unawareness is still under research, it is thought that these individuals progressively begin to develop fewer adrenergic-type symptoms, resulting in the loss of neuroglycopenic-type symptoms.[16][17] Neuroglycopenic symptoms are caused by low glucose in the brain, and can result in tiredness, confusion, difficulty with speech, seizures, and loss of consciousness.[3] Adrenergic symptoms are caused by the body's reaction to low glucose in the brain, and can result in fast heart rate, sweating, nervousness, and hunger.[3] See section above on Signs and Symptoms for further explanation of neuroglycopenic symptoms and adrenergic symptoms.
In terms of epidemiology, hypoglycemic unawareness occurs in 20–40% of type 1 diabetics.[15][17][18]
Other causes
[edit]Other causes of hypoglycemia in diabetics include the following:
- Fasting, whether it be a planned fast or overnight fast, as there is a long period of time without glucose intake[1][3]
- Exercising more than usual as it leads to more use of glucose, especially by the muscles[1][3]
- Drinking alcohol, especially when combined with diabetic medications, as alcohol inhibits glucose production[1][3]
- Kidney disease, as insulin cannot be cleared out of circulation well[3]
Non-diabetics
[edit]Serious illness
[edit]Serious illness may result in low blood sugar.[1][3][2][19] Severe disease of many organ systems can cause hypoglycemia as a secondary problem.[3][2] Hypoglycemia is especially common in those in the intensive care unit or those in whom food and drink is withheld as a part of their treatment plan.[3][19]
Sepsis, a common cause of hypoglycemia in serious illness, can lead to hypoglycemia through many ways.[3][19] In a state of sepsis, the body uses large amounts of glucose for energy.[3][19] Glucose use is further increased by cytokine production.[3] Cytokines are a protein produced by the body in a state of stress, particularly when fighting an infection.[3] Cytokines may inhibit glucose production, further decreasing the body's energy stores.[3] Finally, the liver and kidneys are sites of glucose production, and in a state of sepsis those organs may not receive enough oxygen, leading to decreased glucose production due to organ damage.[3]
Other causes of serious illness that may cause hypoglycemia include liver failure and kidney failure.[3][19] The liver is the main site of glucose production in the body, and any liver failure or damage will lead to decreased glucose production.[3][19] While the kidneys are also sites of glucose production, their failure of glucose production is not significant enough to cause hypoglycemia.[3] Instead, the kidneys are responsible for removing insulin from the body, and when this function is impaired in kidney failure, the insulin stays in circulation longer, leading to hypoglycemia.[3]
Drugs
[edit]A number of medications have been identified which may cause hypoglycemia, through a variety of ways.[3][2][20] Moderate quality evidence implicates the non-steroidal anti-inflammatory drug indomethacin and the anti-malarial quinine.[3][2][20] Low quality evidence implicates lithium, used for bipolar disorder.[2][20] Finally, very low quality evidence implicates a number of hypertension medications including angiotensin converting enzyme inhibitors (also called ACE-inhibitors), angiotensin receptor blockers (also called ARBs), and β-adrenergic blockers (also called beta blockers).[3][2][20] Other medications with very low quality evidence include the antibiotics levofloxacin and trimethoprim-sulfamethoxazole, progesterone blocker mifepristone, anti-arrhythmic disopyramide, anti-coagulant heparin, and chemotherapeutic mercaptopurine.[2][20]
If a person without diabetes accidentally takes medications that are traditionally used to treat diabetes, this may also cause hypoglycemia.[3][2] These medications include insulin, glinides, and sulfonylureas.[3][2] This may occur through medical errors in a healthcare setting or through pharmacy errors, also called iatrogenic hypoglycemia.[3]
Surreptitious insulin use
[edit]When individuals take insulin without needing it, to purposefully induce hypoglycemia, this is referred to as surreptitious insulin use or factitious hypoglycemia.[3][2][21] Some people may use insulin to induce weight loss, whereas for others this may be due to malingering or factitious disorder, which is a psychiatric disorder.[21] Inappropriate usage of insulin is most common in people who have had exposure to diabetes management, such as healthcare workers, people who have relatives with diabetes, or people with diabetes themselves.[3][21] The classic way to identify surreptitious insulin use is through blood work revealing high insulin levels with low C-peptide and proinsulin.[3][21]
Alcohol misuse
[edit]The production of glucose is blocked by alcohol.[3] In those who misuse alcohol, hypoglycemia may be brought on by a several-day alcohol binge associated with little to no food intake.[1][3] The cause of hypoglycemia is multifactorial, where glycogen becomes depleted in a state of starvation.[3] Glycogen stores are then unable to be repleted due to the lack of food intake, all compounded the inhibition of glucose production by alcohol.[3]
Hormone deficiency
[edit]Children with primary adrenal failure, also called Addison's disease, may experience hypoglycemia after long periods of fasting.[3] Addison's disease is associated with chronically low levels of the stress hormone cortisol, which leads to decreased glucose production.[3]
Hypopituitarism, leading to decreased growth hormone, is another cause of hypoglycemia in children, particularly with long periods of fasting or increased exercise.[3]
Inborn errors of metabolism
[edit]Briefly, inborn errors of metabolism are a group of rare genetic disorders that are associated with the improper breakdown or storage of proteins, carbohydrates, or fatty acids.[22] Inborn errors of metabolism may cause infant hypoglycemia, and much less commonly adult hypoglycemia.[22]
Disorders that are related to the breakdown of glycogen, called glycogen storage diseases, may cause hypoglycemia.[3][22] Normally, breakdown of glycogen leads to increased glucose levels, particularly in a fasting state.[3] In glycogen storage diseases, however, glycogen cannot be properly broken down, leading to inappropriately decreased glucose levels in a fasting state, and thus hypoglycemia.[3] The glycogen storage diseases associated with hypoglycemia include type 0, type I, type III, and type IV, as well as Fanconi syndrome.[3]
Some organic and amino acid acidemias, especially those involving the oxidation of fatty acids, can lead to the symptom of intermittent hypoglycemia,[23][24] as for example in combined malonic and methylmalonic aciduria (CMAMMA),[25][26][27] propionic acidemia,[28][23] or isolated methylmalonic acidemia.[28][23]
Insulinomas
[edit]A primary B-cell tumor, such as an insulinoma, is associated with hypoglycemia.[3] This is a tumor located in the pancreas.[3] An insulinoma produces insulin, which in turn decreases glucose levels, causing hypoglycemia.[3] Normal regulatory mechanisms are not in place, which prevent insulin levels from falling during states of low blood glucose.[3] During an episode of hypoglycemia, plasma insulin, C-peptide, and proinsulin will be inappropriately high.[3]
Non-B cell tumors
[edit]Hypoglycemia may occur in people with non-B cell tumors such as hepatomas, adrenocorticoid carcinomas,[29] and carcinoid tumors.[3] These tumors lead to a state of increased insulin, specifically increased insulin-like growth factor II, which decreases glucose levels.[3]
Post-gastric bypass postprandial hypoglycemia
[edit]The Roux-en-Y gastric bypass, is a weight-loss surgery performed on the stomach, and has been associated with hypoglycemia, called post-gastric bypass postprandial hypoglycemia.[3] Although the entire mechanism of hypoglycemia following this surgery is not fully understood, it is thought that meals cause very high levels of glucagon-like peptide-1 (also called GLP-1), a hormone that increases insulin, causing glucose levels to drop.[3]
Autoimmune hypoglycemia
[edit]Antibodies can be formed against insulin, leading to autoimmune hypoglycemia.[3][30] Antibodies are immune proteins produced by the body, that normally attack bacteria and viruses, but sometimes can attack normal human cells, leading to an autoimmune disorder.[31] In autoimmune hypoglycemia, there are two possible mechanisms.[3][30] In one instance, antibodies bind to insulin following its release associated with a meal, resulting in insulin being non-functional.[3][30] At a later time, the antibodies fall off insulin, causing insulin to be functional again leading late hypoglycemia after a meal, called late postprandial hypoglycemia.[3][30] Another mechanism causing hypoglycemia is due to antibodies formed against insulin receptors, called insulin receptor antibodies.[3][30] The antibodies attach to insulin receptors and prevent insulin breakdown, or degradation, leading to inappropriately high insulin levels and low glucose levels.[3][30]
Neonatal hypoglycemia
[edit]Low blood sugar may occur in healthy neonates aged less than 48 hours who have not eaten for a few hours.[8] During the 48-hour neonatal period, the neonate adjusts glucagon and epinephrine levels following birth, which may trigger transient hypoglycemia.[8] In children who are aged greater than 48 hours, serum glucose on average ranges from 70 to 100 mg/dL (3.9–5.5 mmol/L), similar to adults, with hypoglycemia being far less common.[8]
Pathophysiology
[edit]Glucose is the main source of energy for the brain, and a number of mechanisms are in place to prevent hypoglycemia and protect energy supply to the brain.[3][19] The body can adjust insulin production and release, adjust glucose production by the liver, and adjust glucose use by the body.[3][19] The body naturally produces the hormone insulin, in an organ called the pancreas.[3] Insulin helps to regulate the amount of glucose in the body, especially after meals.[3] Glucagon is another hormone involved in regulating blood glucose levels, and can be thought of as the opposite of insulin.[3] Glucagon helps to increase blood glucose levels, especially in states of hunger.[3]
When blood sugar levels fall to the low-normal range, the first line of defense against hypoglycemia is decreasing insulin release by the pancreas.[3][19] This drop in insulin allows the liver to increase glycogenolysis.[3][19] Glycogenolysis is the process of glycogen breakdown that results in the production of glucose.[3][19] Glycogen can be thought of as the inactive, storage form of glucose.[3] Decreased insulin also allows for increased gluconeogenesis in the liver and kidneys.[3][19] Gluconeogenesis is the process of glucose production from non-carbohydrate sources, supplied from muscles and fat.[3][19]
Once blood glucose levels fall out of the normal range, additional protective mechanisms work to prevent hypoglycemia.[3][19] The pancreas is signaled to release glucagon, a hormone that increases glucose production by the liver and kidneys, and increases muscle and fat breakdown to supply gluconeogenesis.[3][32] If increased glucagon does not raise blood sugar levels to normal, the adrenal glands release epinephrine.[3][19] Epinephrine works to also increase gluconeogenesis and glycogenolysis, while also decreasing the use of glucose by organs, protecting the brain's glucose supply.[3][19]
After hypoglycemia has been prolonged, cortisol and growth hormone are released to continue gluconeogenesis and glycogenolysis, while also preventing the use of glucose by other organs.[3][19] The effects of cortisol and growth hormone are far less effective than epinephrine.[3][19] In a state of hypoglycemia, the brain also signals a sense of hunger and drives the person to eat, in an attempt to increase glucose.[3][19]
Diagnosis
[edit]The most reliable method of identifying hypoglycemia is through identifying Whipple's triad.[3][2] The components of Whipple's triad are a blood sugar level below 70 mg/dL (3.9 mmol/L), symptoms related to low blood sugar, and improvement of symptoms when blood sugar is restored to normal.[3][2] Identifying Whipple's triad in a patient helps to avoid unnecessary diagnostic testing and decreases healthcare costs.[2]
In those with a history of diabetes treated with insulin, glinides, or sulfonylurea, who demonstrate Whipple's triad, it is reasonable to assume the cause of hypoglycemia is due to insulin, glinides, or sulfonylurea use.[2] In those without a history of diabetes with hypoglycemia, further diagnostic testing is necessary to identify the cause.[2] Testing, during an episode of hypoglycemia, should include the following:
- Plasma glucose level, not point-of-care measurement[3][2]
- Insulin level[3][2]
- C-peptide level[3][2]
- Proinsulin level[3][2]
- Beta-hydroxybutyrate level[3][2]
- Oral hypoglycemic agent screen[2]
- Response of blood glucose level to glucagon[2]
- Insulin antibodies[2]
If necessary, a diagnostic hypoglycemic episode can be produced in an inpatient or outpatient setting.[3] This is called a diagnostic fast, in which a patient undergoes an observed fast to cause a hypoglycemic episode, allowing for appropriate blood work to be drawn.[3] In some, the hypoglycemic episode may be reproduced simply after a missed meal, whereas in others a fast may last up to 72 hours.[3][2]
In those with a suspected insulinoma, imaging is the most reliable diagnostic technique, including ultrasound, computed tomography (CT) imaging, and magnetic resonance imaging (MRI).[3][2]
Differential diagnosis
[edit]Other conditions that may present at the same time as hypoglycemia include the following:
- Alcohol or drug intoxication[2][33]
- Cardiac arrhythmia[2][33]
- Valvular heart disease[2][33]
- Postprandial syndrome[33]
- Hyperthyroidism[33]
- Pheochromocytoma[33]
- Post-gastric bypass hypoglycemia[2][33]
- Generalized anxiety disorder[33]
- Surreptitious insulin use[2][33]
- Lab or blood draw error (lack of antiglycolytic agent in collection tube or during processing)[34][33]
Treatment
[edit]After hypoglycemia in a person is identified, rapid treatment is necessary and can be life-saving.[1] The main goal of treatment is to raise blood glucose back to normal levels, which is done through various ways of administering glucose, depending on the severity of the hypoglycemia, what is on-hand to treat, and who is administering the treatment.[1][3] A general rule used by the American Diabetes Association is the "15-15 Rule," which suggests consuming or administering 15 grams of a carbohydrate, followed by a 15-minute wait and re-measurement of blood glucose level to assess if blood glucose has returned to normal levels.[5]
Self-treatment
[edit]If an individual recognizes the symptoms of hypoglycemia coming on, blood sugar should promptly be measured, and a sugary food or drink should be consumed.[1] The person must be conscious and able to swallow.[1][3] The goal is to consume 10–20 grams of a carbohydrate to raise blood glucose levels to a minimum of 70 mg/dL (3.9 mmol/L).[3][2]
Examples of products to consume are:
- Glucose tabs or gel (refer to instructions on packet)[1][2]
- Juice containing sugar like apple, grape, or cranberry juice, 1/2 cup (~120 mL)[1][2]
- Soda or a soft-drink, 1/2 cup (~120 mL) (not diet soda)[2]
- Candy[2]
- Table sugar or honey, 1 tbsp (15 mL)[1]
Improvement in blood sugar levels and symptoms are expected to occur in 15–20 minutes, at which point blood sugar should be measured again.[3][2] If the repeat blood sugar level is not above 70 mg/dL (3.9 mmol/L), consume another 10–20 grams of a carbohydrate and remeasure blood sugar levels after 15–20 minutes.[3][2] Repeat until blood glucose levels have returned to normal levels.[3][2] The greatest improvements in blood glucose will be seen if the carbohydrate is chewed or drunk, and then swallowed.[35] This results in the greatest bioavailability of glucose, meaning the greatest amount of glucose enters the body producing the best possible improvements in blood glucose levels.[35] A 2019 systematic review suggests, based on very limited evidence, that oral administration of glucose leads to a bigger improvement in blood glucose levels when compared to buccal administration.[36] This same review reported that, based on limited evidence, no difference was found in plasma glucose when administering combined oral and buccal glucose (via dextrose gel) compared to only oral administration.[36] The second best way to consume a carbohydrate it to allow it to dissolve under the tongue, also referred to as sublingual administration.[35] For example, a hard candy can be dissolved under the tongue, however the best improvements in blood glucose will occur if the hard candy is chewed and crushed, then swallowed.[35]
After correcting blood glucose levels, people may consume a full meal within one hour to replenish glycogen stores.[2]
Education
[edit]Family, friends, and co-workers of a person with diabetes may provide life-saving treatment in the case of a hypoglycemic episode.[1] It is important for these people to receive training on how to recognize hypoglycemia, what foods to help the hypoglycemic eat, how to administer injectable or intra-nasal glucagon, and how to use a glucose meter.[1]

Treatment by family, friends, or co-workers
[edit]Family, friends, and co-workers of those with hypoglycemia are often first to identify hypoglycemic episodes, and may offer help.[3] Upon recognizing the signs and symptoms of hypoglycemia in a diabetic, a blood sugar level should first be measured using a glucose meter.[1] If blood glucose is below 70 mg/dL (3.9 mmol/L), treatment will depend on whether the person is conscious and can swallow safely.[3][2] If the person is conscious and able to swallow, the family, friend, or co-worker can help the hypoglycemic consume 10–20 grams of a carbohydrate to raise blood glucose levels to a minimum of 70 mg/dL (3.9 mmol/L).[2] Improvement in blood sugar level and symptoms is expected to occur in 15–20 minutes, at which point blood sugar is measured again.[3][2] If the repeat blood sugar level is not above 70 mg/dL (3.9 mmol/L), the hypoglycemic should consume another 10–20 grams of a carbohydrate and with remeasurement of blood sugar levels after 15–20 minutes.[3][2] Repeat until blood glucose levels have returned to normal levels, or call emergency services for further assistance.[2]
If the person is unconscious, a glucagon kit may be used to treat severe hypoglycemia, which delivers glucagon either by injection into a muscle or through nasal inhalation.[2][3][19] In the United States, glucacon kits are available by prescription for diabetic patients to carry in case of an episode of severe hypoglycemia.[37][38] Emergency services should be called for further assistance.[2]
Treatment by medical professionals
[edit]In a healthcare setting, treatment depends on the severity of symptoms and intravenous access.[39] If a patient is conscious and able to swallow safely, food or drink may be administered, as well as glucose tabs or gel.[39] In those with intravenous access, 25 grams of 50% dextrose is commonly administered.[39] When there is no intravenous access, intramuscular or intra-nasal glucagon may be administered.[39]
Other treatments
[edit]While the treatment of hypoglycemia is typically managed with carbohydrate consumption, glucagon injection, or dextrose administration, there are some other treatments available.[3] Medications like diazoxide and octreotide decrease insulin levels, increasing blood glucose levels.[3] Dasiglucagon was approved for medical use in the United States in March 2021, to treat severe hypoglycemia.[40] Dasiglucagon (brand name Zegalogue) is unique because it is glucagon in a prefilled syringe or auto-injector pen, as opposed to traditional glucagon kits that require mixing powdered glucagon with a liquid.[40]
Due to its original formulation containing large amounts of glucose, the soft drink Lucozade was recommended by diabetes charities in the United Kingdom as an immediate treatment for hypoglycemia; however, as the drink was reformulated to replace much of its glucose content with artificial sweeteners, this is no longer recommended.[41]
Prevention
[edit]
Diabetics
[edit]The prevention of hypoglycemia depends on the cause.[1][3][2] In those with diabetes treated by insulin, glinides, or sulfonylurea, the prevention of hypoglycemia has a large focus on patient education and medication adjustments.[1][3][2] The foundation of diabetes education is learning how to recognize the signs and symptoms of hypoglycemia, as well as learning how to act quickly to prevent worsening of an episode.[2] Another cornerstone of prevention is strong self-monitoring of blood glucose, with consistent and frequent measurements.[2] Research has shown that patients with type 1 diabetes who use continuous glucose monitoring systems with insulin pumps significantly improve blood glucose control.[42][43][44] Insulin pumps help to prevent high glucose spikes, and help prevent inappropriate insulin dosing.[43][44][45] Continuous glucose monitors can sound alarms when blood glucose is too low or too high, especially helping those with nocturnal hypoglycemia or hypoglycemic unawareness.[43][44][45] In terms of medication adjustments, medication doses and timing can be adjusted to prevent hypoglycemia, or a medication can be stopped altogether.[3][2]
Non-diabetics
[edit]In those with hypoglycemia who do not have diabetes, there are a number of preventative measures dependent on the cause.[1][3][2] Hypoglycemia caused by hormonal dysfunction like lack of cortisol in Addison's disease or lack of growth hormone in hypopituitarism can be prevented with appropriate hormone replacement.[3][2] The hypoglycemic episodes associated with non-B cell tumors can be decreased following surgical removal of the tumor, as well as following radiotherapy or chemotherapy to reduce the size of the tumor.[3][2] In some cases, those with non-B cell tumors may have hormone therapy with growth hormone, glucocorticoid, or octreotide to also lessen hypoglycemic episodes.[3][2] Post-gastric bypass hypoglycemia can be prevented by eating smaller, more frequent meals, avoiding sugar-filled foods, as well as medical treatment with an alpha-glucosidase inhibitor, diazoxide, or octreotide.[3][2]
Some causes of hypoglycemia require treatment of the underlying cause to best prevent hypoglycemia.[2] This is the case for insulinomas which often require surgical removal of the tumor for hypoglycemia to remit.[2] In patients who cannot undergo surgery for removal of the insulinoma, diazoxide or octreotide may be used.[2]
Epidemiology
[edit]Hypoglycemia is common in people with type 1 diabetes, and in people with type 2 diabetes taking insulin, glinides, or sulfonylurea.[1][3] It is estimated that type 1 diabetics experience two mild, symptomatic episodes of hypoglycemia per week.[3] Additionally, people with type 1 diabetes have at least one severe hypoglyemic episode per year, requiring treatment assistance.[3] In terms of mortality, hypoglycemia causes death in 6–10% of type 1 diabetics.[3][verification needed]
In those with type 2 diabetes, hypoglycemia is less common compared to type 1 diabetics, because medications that treat type 2 diabetes like metformin, glitazones, alpha-glucosidase inhibitors, glucagon-like peptide 1 agonists, and dipeptidyl peptidase IV inhibitors, do not cause hypoglycemia.[1][3] Hypoglycemia is common in type 2 diabetics who take insulin, glinides, or sulfonylurea.[1][3] Insulin use remains a key risk factor in developing hypoglycemia, regardless of diabetes type.[1][3]
History
[edit]Hypoglycemia was first discovered by James Collip when he was working with Frederick Banting on purifying insulin in 1922.[46] Collip was asked to develop an assay to measure the activity of insulin.[46] He first injected insulin into a rabbit, and then measured the reduction in blood-glucose levels.[46] Measuring blood glucose was a time-consuming step.[46] Collip observed that if he injected rabbits with a too large a dose of insulin, the rabbits began convulsing, went into a coma, and then died.[46] This observation simplified his assay.[46] He defined one unit of insulin as the amount necessary to induce this convulsing hypoglycemic reaction in a rabbit.[46] Collip later found he could save money, and rabbits, by injecting them with glucose once they were convulsing.[46]
Etymology
[edit]The word hypoglycemia is also spelled hypoglycaemia or hypoglycæmia. The term means 'low blood sugar' from Greek ὑπογλυκαιμία, from ὑπο- hypo- 'under' + γλυκύς glykys 'sweet' + αἷμᾰ haima 'blood'.[47]
References
[edit]- ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj ak National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). "Low Blood Glucose (Hypoglycemia)". NIDDK.nih.gov. Archived from the original on 28 July 2017. Retrieved 12 January 2022.
- ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj ak al am an ao ap aq ar as at au av aw ax ay az ba bb bc bd be bf bg bh bi bj bk bl bm bn bo bp bq br bs bt bu bv bw bx by bz ca cb cc cd ce cf cg ch Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, Service FJ (March 2009). "Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline". The Journal of Clinical Endocrinology and Metabolism. 94 (3): 709–728. doi:10.1210/jc.2008-1410. PMID 19088155.
- ^ a b c d e f g h i j k l m n o p q r s t u v w x y z aa ab ac ad ae af ag ah ai aj ak al am an ao ap aq ar as at au av aw ax ay az ba bb bc bd be bf bg bh bi bj bk bl bm bn bo bp bq br bs bt bu bv bw bx by bz ca cb cc cd ce cf cg ch ci cj ck cl cm cn co cp cq cr cs ct cu cv cw cx cy cz da db dc dd de df dg dh di dj dk dl dm dn do dp dq dr ds dt du dv dw dx dy dz ea eb ec ed ee ef eg eh ei ej ek el em en Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J (2018). Harrison's principles of internal medicine (20th ed.). New York. ISBN 978-1-259-64403-0. OCLC 1029074059.
{{cite book}}: CS1 maint: location missing publisher (link) - ^ a b c Young VB (2016). Blueprints medicine. William A. Kormos, Davoren A. Chick (6th ed.). Philadelphia. ISBN 978-1-4698-6415-0. OCLC 909025539.
{{cite book}}: CS1 maint: location missing publisher (link) - ^ a b c d e f g American Diabetes Association (ADA). "Hypoglycemia (Low Blood Glucose)". www.diabetes.org. Archived from the original on 13 January 2022. Retrieved 12 January 2022.
- ^ a b c Yanai H, Adachi H, Katsuyama H, Moriyama S, Hamasaki H, Sako A (February 2015). "Causative anti-diabetic drugs and the underlying clinical factors for hypoglycemia in patients with diabetes". World Journal of Diabetes. 6 (1): 30–36. doi:10.4239/wjd.v6.i1.30. PMC 4317315. PMID 25685276.
- ^ "Treatment of hypoglycaemia in children with severe acute malnutrition". www.who.int. Retrieved 6 December 2024.
- ^ a b c d e f g h i j k l Thornton PS, Stanley CA, De Leon DD, Harris D, Haymond MW, Hussain K, et al. (August 2015). "Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children". The Journal of Pediatrics. 167 (2): 238–245. doi:10.1016/j.jpeds.2015.03.057. PMC 11891912. PMID 25957977. S2CID 10681217.
- ^ "FDA approves first treatment for severe hypoglycemia that can be administered without an injection". FDA. 11 September 2019. Archived from the original on 17 May 2020. Retrieved 11 November 2019.
- ^ Mathew P, Thoppil D (2024), "Hypoglycemia", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30521262, retrieved 16 August 2024
- ^ "Low Blood Sugar (Hypoglycemia)". diabetesdaily.com. 8 August 2021.
- ^ Ling S, Zaccardi F, Lawson C, Seidu SI, Davies MJ, Khunti K (1 April 2021). "Glucose Control, Sulfonylureas, and Insulin Treatment in Elderly People With Type 2 Diabetes and Risk of Severe Hypoglycemia and Death: An Observational Study". Diabetes Care. 44 (4): 915–924. doi:10.2337/dc20-0876. ISSN 1935-5548. PMID 33541857.
- ^ "Hangry is officially a word in the Oxford English Dictionary". ABC News. Retrieved 6 January 2024.
- ^ "If you've ever been hangry, this is what your body may be telling you". Washington Post. 9 July 2018. ISSN 0190-8286. Retrieved 6 January 2024.
- ^ a b c d e f g Johnson-Rabbett B, Seaquist ER (September 2019). "Hypoglycemia in diabetes: The dark side of diabetes treatment. A patient-centered review". Journal of Diabetes. 11 (9): 711–718. doi:10.1111/1753-0407.12933. PMID 30983138. S2CID 115202581.
- ^ a b c d e f g Ibrahim M, Baker J, Cahn A, Eckel RH, El Sayed NA, Fischl AH, et al. (November 2020). "Hypoglycaemia and its management in primary care setting" (PDF). Diabetes/Metabolism Research and Reviews. 36 (8) e3332. doi:10.1002/dmrr.3332. PMID 32343474. S2CID 216594548.
- ^ a b c d e f g h Martín-Timón I, Del Cañizo-Gómez FJ (July 2015). "Mechanisms of hypoglycemia unawareness and implications in diabetic patients". World Journal of Diabetes. 6 (7): 912–926. doi:10.4239/wjd.v6.i7.912. PMC 4499525. PMID 26185599.
- ^ Lucidi P, Porcellati F, Bolli GB, Fanelli CG (August 2018). "Prevention and Management of Severe Hypoglycemia and Hypoglycemia Unawareness: Incorporating Sensor Technology". Current Diabetes Reports. 18 (10) 83. doi:10.1007/s11892-018-1065-6. PMID 30121746. S2CID 52039366.
- ^ a b c d e f g h i j k l m n o p q r s t Mathew P, Thoppil D (2022). "Hypoglycemia". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 30521262. Archived from the original on 30 August 2021. Retrieved 24 January 2022.
- ^ a b c d e Murad MH, Coto-Yglesias F, Wang AT, Sheidaee N, Mullan RJ, Elamin MB, et al. (March 2009). "Clinical review: Drug-induced hypoglycemia: a systematic review". The Journal of Clinical Endocrinology and Metabolism. 94 (3): 741–745. doi:10.1210/jc.2008-1416. PMID 19088166.
- ^ a b c d Awad DH, Gokarakonda SB, Ilahi M (2022). "Factitious Hypoglycemia". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 31194450. Archived from the original on 26 January 2022. Retrieved 21 January 2022.
- ^ a b c Jeanmonod R, Asuka E, Jeanmonod D (2022). "Inborn Errors Of Metabolism". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 29083820. Archived from the original on 13 October 2021. Retrieved 24 January 2022.
- ^ a b c Ozand PT (2000). "Hypoglycemia in association with various organic and amino acid disorders". Seminars in Perinatology. 24 (2): 172–193. doi:10.1053/sp.2000.6367. PMID 10805172.
- ^ Baker JJ, Burton BK (November 2021). "Diagnosis and Clinical Management of Long-chain Fatty-acid Oxidation Disorders: A Review". TouchREVIEWS in Endocrinology. 17 (2): 108–111. doi:10.17925/EE.2021.17.2.108. ISSN 2752-5457. PMC 8676101. PMID 35118456.
- ^ NIH Intramural Sequencing Center Group, Sloan JL, Johnston JJ, Manoli I, Chandler RJ, Krause C, Carrillo-Carrasco N, Chandrasekaran SD, Sysol JR, O'Brien K, Hauser NS, Sapp JC, Dorward HM, Huizing M, Barshop BA (2011). "Exome sequencing identifies ACSF3 as a cause of combined malonic and methylmalonic aciduria". Nature Genetics. 43 (9): 883–886. doi:10.1038/ng.908. ISSN 1061-4036. PMC 3163731. PMID 21841779.
- ^ Wehbe Z, Behringer S, Alatibi K, Watkins D, Rosenblatt D, Spiekerkoetter U, Tucci S (2019). "The emerging role of the mitochondrial fatty-acid synthase (mtFASII) in the regulation of energy metabolism". Biochimica et Biophysica Acta (BBA) - Molecular and Cell Biology of Lipids. 1864 (11): 1629–1643. doi:10.1016/j.bbalip.2019.07.012. PMID 31376476. S2CID 199404906.
- ^ Levtova A, Waters PJ, Buhas D, Lévesque S, Auray-Blais C, Clarke JT, Laframboise R, Maranda B, Mitchell GA, Brunel-Guitton C, Braverman NE (2019). "Combined malonic and methylmalonic aciduria due to ACSF3 mutations: Benign clinical course in an unselected cohort". Journal of Inherited Metabolic Disease. 42 (1): 107–116. doi:10.1002/jimd.12032. ISSN 0141-8955. PMID 30740739. S2CID 73436689.
- ^ a b Ozand PT, Al-Essa M (2012), Elzouki AY, Harfi HA, Nazer HM, Stapleton FB (eds.), "Disorders of Organic Acid and Amino Acid Metabolism", Textbook of Clinical Pediatrics, Berlin, Heidelberg: Springer Berlin Heidelberg, pp. 451–514, doi:10.1007/978-3-642-02202-9_38, ISBN 978-3-642-02201-2
- ^ "Adrenocortical Carcinoma Treatment - NCI". www.cancer.gov. 6 July 2007. Retrieved 16 August 2024.
- ^ a b c d e f Lupsa BC, Chong AY, Cochran EK, Soos MA, Semple RK, Gorden P (May 2009). "Autoimmune forms of hypoglycemia". Medicine. 88 (3): 141–153. doi:10.1097/MD.0b013e3181a5b42e. PMID 19440117. S2CID 34429211.
- ^ "Antibody". Genome.gov. Archived from the original on 9 October 2020. Retrieved 24 January 2022.
- ^ Rix I, Nexøe-Larsen C, Bergmann NC, Lund A, Knop FK (2000). "Glucagon Physiology". In Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, et al. (eds.). Endotext. PMID 25905350. Archived from the original on 15 January 2021.
- ^ a b c d e f g h i j Vella A. "Hypoglycemia in adults without diabetes mellitus: Clinical manifestations, diagnosis, and causes". www.uptodate.com. Archived from the original on 26 January 2022. Retrieved 14 January 2022.
- ^ "Low Blood Glucose (Hypoglycemia) - NIDDK". National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved 16 August 2024.
- ^ a b c d De Buck E, Borra V, Carlson JN, Zideman DA, Singletary EM, Djärv T (April 2019). "First aid glucose administration routes for symptomatic hypoglycaemia". The Cochrane Database of Systematic Reviews. 2019 (4) CD013283. doi:10.1002/14651858.cd013283.pub2. PMC 6459163. PMID 30973639.
- ^ a b De Buck E, Borra V, Carlson JN, Zideman DA, Singletary EM, Djärv T, et al. (Cochrane Metabolic and Endocrine Disorders Group) (April 2019). "First aid glucose administration routes for symptomatic hypoglycaemia". The Cochrane Database of Systematic Reviews. 2019 (4) CD013283. doi:10.1002/14651858.CD013283.pub2. PMC 6459163. PMID 30973639.
- ^ "Severe Low Blood Sugar (Hypoglycemia) Treatment | Lilly GLUCAGON". www.lillyglucagon.com. Archived from the original on 24 January 2022. Retrieved 24 January 2022.
- ^ "Glucacon Emergency Kit". Glucagon Emergency Kit. Archived from the original on 24 January 2022. Retrieved 24 January 2022.
- ^ a b c d Pasala S, Dendy JA, Chockalingam V, Meadows RY (2013). "An inpatient hypoglycemia committee: development, successful implementation, and impact on patient safety". The Ochsner Journal. 13 (3): 407–412. PMC 3776519. PMID 24052773.
- ^ a b "HIGHLIGHTS OF PRESCRIBING INFORMATION. These highlights do not include all the information needed to use ZEGALOGUE® safely and effectively. See full prescribing information for ZEGALOGUE. ZEGALOGUE (dasiglucagon) injection, for subcutaneous use" (PDF). Accessdate.fsa.gov. Archived from the original (PDF) on 15 May 2021. Retrieved 10 November 2021.
- ^ Harrold A. "Diabetic patients should be warned about changes to Lucozade glucose content". Nursing in Practice. Archived from the original on 28 February 2019. Retrieved 27 February 2019.
- ^ Langendam M, Luijf YM, Hooft L, Devries JH, Mudde AH, Scholten RJ (January 2012). "Continuous glucose monitoring systems for type 1 diabetes mellitus". The Cochrane Database of Systematic Reviews. 1 (1) CD008101. doi:10.1002/14651858.cd008101.pub2. PMC 6486112. PMID 22258980.
- ^ a b c Azhar A, Gillani SW, Mohiuddin G, Majeed RA (2020). "A systematic review on clinical implication of continuous glucose monitoring in diabetes management". Journal of Pharmacy & Bioallied Sciences. 12 (2): 102–111. doi:10.4103/jpbs.JPBS_7_20. PMC 7373113. PMID 32742108.
- ^ a b c Mian Z, Hermayer KL, Jenkins A (November 2019). "Continuous Glucose Monitoring: Review of an Innovation in Diabetes Management". The American Journal of the Medical Sciences. 358 (5): 332–339. doi:10.1016/j.amjms.2019.07.003. PMID 31402042. S2CID 199047204.
- ^ a b "Continuous Glucose Monitoring | NIDDK". National Institute of Diabetes and Digestive and Kidney Diseases. Archived from the original on 12 January 2022. Retrieved 25 January 2022.
- ^ a b c d e f g h "Collip discovers hypoglycemia". Treating Diabetes. Archived from the original on 8 September 2017. Retrieved 18 June 2017.
- ^ "Non-Diabetic Hypoglycemia | Causes, Symptoms & Treatment". study.com. 21 November 2023. Retrieved 16 August 2024.
External links
[edit]- Hypoglycemia at the Mayo Clinic
- American Diabetes Association
- "Hypoglycemia". MedlinePlus. U.S. National Library of Medicine.
Hypoglycemia
View on GrokipediaDefinition and Classification
Definition
Hypoglycemia is defined as a plasma glucose concentration below 70 mg/dL (3.9 mmol/L), which represents the threshold for level 1 hypoglycemia in individuals with diabetes, as established by the American Diabetes Association (ADA).[5] Level 2 hypoglycemia occurs at concentrations below 54 mg/dL (3.0 mmol/L), indicating a more clinically significant decline that may require immediate intervention, while level 3, or severe hypoglycemia, is characterized by glucose levels low enough to cause altered mental status or require assistance from another person for recovery.[5] These thresholds were initially formalized in the ADA's 2005 Workgroup report, which set 70 mg/dL as a conservative limit based on physiological responses in nondiabetic individuals, and have been refined in subsequent standards of care to better reflect clinical risk.[6] In contrast to euglycemia, where plasma glucose levels typically range from 70 to 140 mg/dL and adequately support energy demands, hypoglycemia disrupts the primary fuel supply to glucose-dependent tissues, particularly the brain, which relies almost exclusively on glucose for energy metabolism and cannot effectively utilize alternative substrates like fatty acids under acute conditions.[7] Hyperglycemia, defined as levels exceeding 180 mg/dL, involves excess glucose availability that can lead to cellular damage over time but does not pose the immediate threat to neuronal function seen in hypoglycemia.[5] The physiological significance of these thresholds is underscored by the initiation of counter-regulatory hormone responses, such as glucagon and epinephrine release, which begin around 65 mg/dL (3.6 mmol/L) in nondiabetic individuals to restore glucose homeostasis by promoting hepatic glycogenolysis and gluconeogenesis.[6] This response aims to prevent progression to severe deficits in cerebral energy supply. Diagnosis of hypoglycemia as a clinical entity is confirmed using Whipple's triad, which links low glucose levels to associated symptoms and their resolution upon glucose restoration.[6]Whipple's Triad
Whipple's triad serves as the foundational diagnostic criteria for confirming that a patient's symptoms are attributable to hypoglycemia. It requires the presence of three interrelated elements: symptoms consistent with low blood sugar, such as neuroglycopenic or autonomic manifestations; documentation of a low plasma glucose concentration at the time of those symptoms, generally defined as below 70 mg/dL (3.9 mmol/L) in clinical contexts; and subsequent resolution of the symptoms following restoration of blood glucose to normal levels, typically through administration of glucose or carbohydrates.[6][8] This structured approach ensures that transient symptoms are not misattributed to hypoglycemia without biochemical and therapeutic corroboration. The triad originated from the work of American surgeon Allen O. Whipple in the 1930s, who introduced it as a clinical tool to differentiate hyperinsulinemic states, particularly those caused by insulinomas—rare pancreatic tumors leading to excessive insulin secretion and recurrent fasting hypoglycemia.[9] Whipple's observations, drawn from surgical cases and metabolic studies, emphasized the need for all three components to guide preoperative diagnosis and intervention in suspected endogenous hyperinsulinism.[10] This framework has since become a cornerstone in endocrinology, extending beyond its initial insulinoma focus to broader applications in hypoglycemia evaluation. In contemporary practice, Whipple's triad is utilized across both diabetic and non-diabetic populations to establish causality between low glucose and symptoms, effectively excluding pseudohypoglycemia—a condition where patients experience hypoglycemic-like symptoms due to rapid glucose fluctuations or other factors, despite normal plasma glucose levels.[11][12] For instance, in non-diabetic patients with suspected spontaneous hypoglycemia, fulfilling the triad during a supervised fast or spontaneous episode supports targeted investigations into underlying etiologies like occult insulinomas or metabolic disorders.[8] Despite advancements in continuous glucose monitoring (CGM) systems, which enable proactive detection of asymptomatic or nocturnal hypoglycemic excursions without relying on patient-reported symptoms, Whipple's triad maintains enduring utility for assessing discrete, symptomatic events where CGM data alone may not capture the full clinical context.[1] CGM's limitations in absolute accuracy during extremes and its focus on trends can complement but not supplant the triad's emphasis on symptom-glucose-response linkage, particularly in resource-limited settings or for validating episodic complaints.[13] Thus, it remains a practical, low-tech benchmark in modern hypoglycemia management.Types and Classification
Hypoglycemia is classified in multiple ways to guide clinical assessment and management, primarily based on its timing relative to meals, severity of symptoms and required intervention, patient age, and whether an underlying pathologic process is identifiable. These categorizations help differentiate clinical presentations and inform diagnostic approaches, with confirmation across types relying on Whipple's triad—documented low blood glucose, associated symptoms, and resolution upon glucose restoration.[1] One key distinction is between fasting and reactive (postprandial) hypoglycemia. Fasting hypoglycemia develops during periods of prolonged abstinence from food, typically after 8 hours or more, and is often indicative of impaired glucose production or excessive consumption, leading to subacute or chronic symptoms such as neuroglycopenia.[14] In contrast, reactive hypoglycemia occurs 2 to 5 hours after a meal, triggered by rapid glucose fluctuations, and commonly presents with acute neurogenic symptoms like sweating, tremors, and anxiety.[15] Severity is graded into three levels based on blood glucose thresholds and clinical impact, a framework adopted by major endocrine organizations for both diabetic and non-diabetic contexts. Level 1 (mild) involves glucose levels below 70 mg/dL (3.9 mmol/L) but at or above 54 mg/dL (3.0 mmol/L), where individuals can typically self-treat with carbohydrates.[5] Level 2 (moderate) is defined by glucose below 54 mg/dL (3.0 mmol/L), often causing neuroglycopenic symptoms and requiring assistance from others for treatment.[16] Level 3 (severe) encompasses events severe enough to impair mental or physical function, necessitating external aid, and may result in unconsciousness, seizures, or life-threatening complications regardless of exact glucose measurement.[5]| Severity Level | Glucose Threshold | Characteristics |
|---|---|---|
| Level 1 (Mild) | <70 mg/dL (3.9 mmol/L) and ≥54 mg/dL (3.0 mmol/L) | Alertness maintained; self-treatment possible with oral carbohydrates.[5] |
| Level 2 (Moderate) | <54 mg/dL (3.0 mmol/L) | Significant symptoms; assistance needed for intervention.[16] |
| Level 3 (Severe) | Any level requiring aid | Altered consciousness or seizures; third-party assistance essential, often with glucagon or IV glucose.[5] |
Epidemiology
In Diabetes
Hypoglycemia is a significant concern in diabetic populations, particularly among those with type 1 diabetes (T1D) and insulin-treated type 2 diabetes (T2D). In T1D, the annual prevalence of severe hypoglycemia—defined as an event requiring assistance for recovery—is estimated at 30–40%, with an incidence of 1.0–1.7 episodes per patient per year.[20] For insulin-treated T2D, rates are generally lower but still substantial, with approximately 25% of patients on insulin for more than five years experiencing severe events annually, and an incidence of around 0.35–2.5 episodes per patient per year.[21] In contrast, the prevalence is much lower among those managed with oral agents like sulfonylureas, affecting less than 1% of patients requiring emergency treatment.[22] Globally, these risks are amplified by the scale of diabetes, with 589 million adults aged 20–79 years living with the condition in 2024, projected to rise to 853 million by 2050.[23] Approximately 81% of these individuals reside in low- and middle-income countries (LMICs), where rates of hypoglycemia are higher due to limited access to glucose monitoring, education, and appropriate therapies, as well as a disproportionate burden of undiagnosed cases (90% of the 252 million undiagnosed adults are in LMICs).[23][5] Key risk factors for hypoglycemia in diabetes include insulin use, which intensifies the likelihood of episodes compared to oral agents.[5] Long disease duration exceeding 13 years further elevates risk, as does renal impairment with an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m², which impairs glucose homeostasis and insulin clearance.[24][25] Trends in hypoglycemia reflect the growing diabetes epidemic, with overall events increasing alongside rising prevalence, yet severe incidents are declining in high-income settings due to advancements like continuous glucose monitoring (CGM) and safer pharmacotherapies such as SGLT2 inhibitors.[5] For instance, in South Korea, the incidence of severe hypoglycemia in T2D peaked at 6.84 per 1,000 person-years in 2012 before falling to 4.43 by 2019, attributed to individualized glycemic targets and reduced use of high-risk agents.[26] More recent data from the US indicate continued declines, with hospitalized hypoglycemia rates among diabetic patients dropping to 6.3% by 2022, a 15% decrease from 2016, partly due to expanded CGM use.[27]In Non-Diabetes
Hypoglycemia in non-diabetic individuals is uncommon, affecting less than 1% of the general population, though it is more frequently observed in specific vulnerable groups such as hospitalized elderly patients or those recovering from surgery.[28][29] In hospitalized non-diabetic adults, the frequency reaches approximately 3.8 per 10,000 admissions, with elderly patients facing a substantially elevated risk due to factors like reduced physiological reserves and comorbidities.[30][31] This rarity contrasts sharply with the much higher burden in diabetic populations, where hypoglycemia events are far more prevalent.[28] Global data on non-diabetic hypoglycemia remain limited, reflecting challenges in systematic reporting and diagnosis. Neonatal incidence is notably higher among at-risk newborns, with estimates of 15% overall in neonates and up to 50% in those with risk factors receiving a hypoglycemia diagnosis under current screening guidelines; up to 30% of newborns may be considered at risk.[32] In adults without diabetes, the annual incidence is very low, often linked to rare underlying conditions or acute insults.[33] These figures underscore the condition's infrequency in community settings but highlight its potential severity when it occurs. Regional variations influence the distribution of non-diabetic hypoglycemia, with higher rates reported in areas characterized by elevated alcohol misuse or chronic malnutrition, where impaired gluconeogenesis and depleted glycogen stores exacerbate vulnerability.[34][35] In low-resource settings, the condition is frequently underdiagnosed due to limited access to blood glucose monitoring and diagnostic facilities, leading to incomplete epidemiological capture.[36] Overall trends in non-diabetic hypoglycemia appear stable in the general population, but there is growing recognition of its increased occurrence following bariatric surgery, affecting up to 30% of patients in certain cohorts, particularly those undergoing procedures like Roux-en-Y gastric bypass.[37][38] This rise is attributed to enhanced post-operative surveillance and awareness of postprandial hypoglycemia as a complication.[39]Pathophysiology
Glucose Homeostasis
Glucose homeostasis refers to the intricate physiological processes that maintain blood glucose levels within a narrow range to ensure a steady energy supply for vital organs. This regulation involves coordinated actions among several key organs and hormones, preventing fluctuations that could impair cellular function. The primary organs include the liver, pancreas, and brain, each playing distinct roles in glucose production, storage, and utilization.[40] The liver serves as the central hub for glucose buffering, primarily through glycogenolysis—the breakdown of stored glycogen into glucose during fasting—and gluconeogenesis, the synthesis of new glucose from non-carbohydrate precursors like lactate and amino acids.[40] In contrast, skeletal muscle also stores glycogen but lacks the enzyme glucose-6-phosphatase, which is required to dephosphorylate glucose-6-phosphate and release free glucose into the circulation. Consequently, muscle glycogen is utilized exclusively for local energy production within muscle cells and does not contribute to systemic blood glucose maintenance, particularly during hypoglycemia.[41] The pancreas, via its endocrine islets, secretes insulin from beta cells to facilitate glucose uptake and storage postprandially, while alpha cells release glucagon to stimulate hepatic glucose release during fasting.[42] Additional counter-regulatory hormones, such as cortisol from the adrenal cortex and epinephrine from the adrenal medulla, further elevate blood glucose by promoting glycogenolysis and inhibiting insulin secretion when levels drop.[43] The brain acts as a critical sensor; its hypothalamus detects declining glucose and triggers sympathetic responses to initiate counter-regulation, ensuring prioritized glucose delivery.[40] These mechanisms operate through negative feedback loops that respond to nutritional states. In the fed (postprandial) state, rising blood glucose prompts insulin secretion, enhancing peripheral uptake in muscle and adipose tissue while suppressing hepatic glucose output, typically keeping levels below 140 mg/dL (7.8 mmol/L). During fasting, falling glucose levels stimulate glucagon, cortisol, and epinephrine, promoting endogenous glucose production to maintain fasting concentrations between 70 and 99 mg/dL (3.9 and 5.5 mmol/L). Overall, these loops sustain blood glucose within 70-140 mg/dL (3.9-7.8 mmol/L) under normal conditions.[44] A key aspect of this homeostasis is the brain's heavy reliance on glucose as its primary fuel, consuming approximately 120 g per day, which accounts for about 20% of total body energy expenditure despite comprising only 2% of body weight.[45] In prolonged fasting, the liver shifts to ketone production from fatty acids as an alternative energy source for the brain, sparing glucose for glucose-dependent tissues like red blood cells.[40] This adaptive mechanism underscores the evolutionary priority of cerebral energy supply in glucose regulation.[43]Mechanisms of Hypoglycemia
Hypoglycemia arises from disruptions in the normal counter-regulatory mechanisms that maintain blood glucose levels, primarily through impaired hepatic glucose production via glycogenolysis and gluconeogenesis. In physiological conditions, a decline in blood glucose triggers the release of counter-regulatory hormones such as glucagon and epinephrine, which stimulate glycogen breakdown and new glucose synthesis in the liver to restore euglycemia. However, excess insulin or suppressed counter-regulatory responses inhibit these processes, leading to inadequate glucose output and subsequent hypoglycemia.[1][46][47] Counter-regulatory hormone deficiencies play a central role in the pathogenesis of hypoglycemia, particularly in recurrent episodes where the responses of epinephrine and glucagon become blunted. Glucagon primarily promotes hepatic glycogenolysis, while epinephrine enhances both glycogenolysis and gluconeogenesis; deficiencies in these hormones reduce glucose mobilization, exacerbating low blood glucose levels. In individuals with frequent hypoglycemic events, prior exposure shifts the glycemic thresholds for these hormonal responses downward, impairing their effectiveness and increasing susceptibility to further episodes.[46][48][49] Neuroglycopenia occurs when brain glucose deprivation reaches critical levels, typically below 50 mg/dL (2.8 mmol/L), due to the blood-brain barrier's reliance on facilitated glucose transport that becomes saturated under low plasma concentrations. This threshold varies slightly but generally marks the point where cerebral glucose utilization outpaces supply, leading to central nervous system dysfunction. The brain's high metabolic demand for glucose underscores the rapid onset of neuroglycopenic effects in severe hypoglycemia.[1][48] A feedback vicious cycle, known as hypoglycemia-associated autonomic failure (HAAF), perpetuates recurrent hypoglycemia through progressive blunting of autonomic and symptomatic responses. Antecedent hypoglycemia desensitizes glucose-sensing mechanisms in the brain, reducing epinephrine secretion and neurogenic warning signs, which in turn allows blood glucose to fall further without detection or correction. This cycle heightens the risk of severe episodes, as diminished awareness prevents timely intervention.[50][51][52]Etiology
Diabetic Causes
The first episode of hypoglycemia in individuals with diabetes is most commonly caused by excessive administration of insulin or oral hypoglycemic agents, insufficient food intake, excessive exercise, or a mismatch between medication, eating, and physical activity. Hypoglycemia in individuals with diabetes primarily arises from therapeutic interventions that disrupt glucose homeostasis, particularly through medications that enhance insulin action or secretion. The most common cause is excessive insulin administration, including overdoses or inappropriate dosing, which leads to an absolute or relative excess of insulin relative to glucose availability. Sulfonylureas, such as glipizide, glimepiride, and glyburide, stimulate endogenous insulin release from pancreatic beta cells, increasing the risk of prolonged hypoglycemia due to their extended duration of action. Similarly, meglitinides like repaglinide and nateglinide promote rapid insulin secretion but can cause hypoglycemia if meals are skipped or doses are miscalculated. Dosing errors, such as misjudging carbohydrate intake or using the wrong type of insulin (e.g., short-acting instead of long-acting), are frequent iatrogenic contributors, affecting up to twice-weekly symptomatic episodes in type 1 diabetes patients. Recurrent episodes of hypoglycemia can lead to hypoglycemia unawareness, a condition where individuals fail to recognize symptoms due to blunted adrenergic responses, such as reduced epinephrine-mediated tachycardia and sweating, stemming from prior exposure to low glucose levels. This autonomic failure increases the vulnerability to severe events, as patients may not adjust behaviors or seek intervention promptly; avoidance of hypoglycemia for 2-3 weeks can reverse this in most cases. Intensive glycemic control, targeting lower HbA1c levels (e.g., below 6.0%), further elevates risk by necessitating tighter medication regimens, with type 1 diabetes patients experiencing 62-170 severe episodes per 100 patient-years under such targets. Additional triggers include lifestyle and physiological factors that exacerbate insulin excess. Unadjusted exercise increases glucose utilization and insulin sensitivity, potentially causing delayed hypoglycemia for hours post-activity, particularly overnight. Skipping or delaying meals reduces exogenous glucose intake, amplifying the effects of administered insulin or secretagogues. Alcohol consumption inhibits hepatic gluconeogenesis, heightening risk especially on an empty stomach or after glycogen depletion, with effects persisting for several hours. Comorbid renal or hepatic impairment impairs insulin clearance and glucose production, respectively, thereby prolonging hypoglycemia in affected patients.Non-Diabetic Causes
Hypoglycemia in individuals without diabetes is a rare but critical condition that typically signals an underlying serious disorder, as healthy counterregulatory mechanisms usually maintain blood glucose levels above 70 mg/dL. A first episode, especially in those without a prior history of diabetes, is less common than in diabetic patients and warrants prompt medical evaluation to identify potential serious underlying conditions such as tumors (e.g., insulinoma) or hormonal deficiencies (e.g., adrenal or pituitary insufficiency) to prevent diagnostic delays. Common causes include excessive alcohol consumption (particularly on an empty stomach), accidental ingestion of diabetes medications belonging to others, serious illnesses (such as liver or kidney failure, severe infections, or critical illness), malnutrition, insulinoma, hormone deficiencies (such as adrenal or pituitary insufficiency), and reactive hypoglycemia following gastric surgery. The etiologies span multiple categories, including critical illnesses that impair glucose production, medications that disrupt homeostasis, endocrine deficiencies, and various metabolic or tumoral abnormalities. Diagnosis requires careful evaluation to distinguish these from iatrogenic causes, with treatment targeting the root pathology.[33] Serious IllnessesCritical conditions such as sepsis, liver failure, renal disease, and heart failure can precipitate hypoglycemia by overwhelming glucose homeostasis. In sepsis, excessive glucose utilization by the host and pathogens, coupled with reduced hepatic glycogenolysis and gluconeogenesis, leads to profound drops in blood glucose, often below 40 mg/dL in severe cases. Liver failure impairs glycogen storage and gluconeogenesis due to hepatocyte dysfunction, resulting in fasting hypoglycemia that may manifest within hours of glucose deprivation. Renal disease, particularly in end-stage renal failure, contributes through decreased clearance of insulin and impaired gluconeogenesis in the kidneys, exacerbating hypoglycemia during illness or malnutrition. Heart failure similarly promotes hypoglycemia via increased glucose consumption by the stressed myocardium and reduced hepatic perfusion, limiting substrate availability for glucose production. These illnesses often present with hypoglycemia as a late, life-threatening complication.[28][53] Drugs and Toxins
Certain non-diabetic medications and substances can induce hypoglycemia through direct effects on insulin secretion or glucose production. Quinine, used for malaria, stimulates endogenous insulin release from pancreatic beta cells, causing postprandial hypoglycemia in susceptible individuals. Pentamidine, an antiprotozoal agent for Pneumocystis pneumonia, damages beta cells and provokes hyperinsulinemia, with hypoglycemia occurring in up to 10-20% of treated patients. Alcohol, particularly in binge drinking, inhibits hepatic gluconeogenesis by depleting NAD+ cofactors and increasing insulin sensitivity, leading to delayed hypoglycemia 6-36 hours after consumption, especially in fasting states. These drug-induced cases are reversible upon discontinuation but require prompt recognition to prevent recurrent episodes.[33][28] Endocrine Disorders
Endocrine deficiencies disrupt counterregulatory hormones essential for glucose maintenance. Adrenal insufficiency, as in Addison's disease, reduces cortisol and aldosterone, impairing gluconeogenesis and increasing insulin sensitivity, which can cause fasting hypoglycemia with symptoms like fatigue and hypotension. Pituitary insufficiency leads to secondary deficiencies in ACTH, growth hormone, and TSH, collectively diminishing glucose production and hepatic enzyme activity, often resulting in hypoglycemia during stress or fasting. Insulinoma, a rare pancreatic beta-cell tumor, causes endogenous hyperinsulinism, with inappropriately elevated insulin levels during hypoglycemia (e.g., insulin >3 μU/mL at glucose <55 mg/dL); incidence is approximately 1-4 per million annually, and surgical resection is curative in 90% of localized cases. These conditions highlight the role of hormonal balance in preventing hypoglycemia.[33][53][54] Other Causes
Inborn errors of metabolism, such as glycogen storage disease (GSD) type 1 (von Gierke disease), result from deficiencies in glucose-6-phosphatase, preventing hepatic glucose release and causing severe fasting hypoglycemia within 3-4 hours, accompanied by lactic acidosis and hepatomegaly. Recent advances in genetic screening, including next-generation sequencing panels, have improved early diagnosis of GSD type 1 variants (e.g., G6PC gene mutations), enabling presymptomatic intervention per American College of Medical Genetics and Genomics practice guideline (2014).[55] Post-gastric bypass surgery, particularly Roux-en-Y, induces reactive postprandial hypoglycemia in 10-30% of patients due to rapid nutrient absorption and exaggerated incretin-driven insulin secretion. Autoimmune hypoglycemia, as in insulin autoimmune syndrome, involves antibodies binding insulin, causing erratic release and hypoglycemia, often triggered by drugs like methimazole. In neonates without maternal diabetes, prematurity and inborn errors (e.g., hereditary fructose intolerance) contribute via immature gluconeogenesis or metabolic blocks, with reported incidences ranging from 20% to 60% in preterm infants.[56] Non-islet cell tumors, such as mesenchymal sarcomas, produce IGF-2, which suppresses growth hormone and mimics insulin action, leading to fasting hypoglycemia in 4-7% of large tumor cases. Surreptitious insulin administration, often in factitious disorder, elevates serum insulin while suppressing C-peptide, mimicking insulinoma but detectable via exogenous insulin assays. These diverse etiologies underscore the need for comprehensive metabolic evaluation.[28][57][33][54]
Clinical Presentation
Symptoms
Hypoglycemia manifests through two primary categories of symptoms: adrenergic (or neurogenic) and neuroglycopenic, which arise due to the body's physiological responses to low blood glucose levels. Adrenergic symptoms typically occur early as a warning mechanism, triggered by catecholamine release, while neuroglycopenic symptoms reflect direct effects of glucose deprivation on the central nervous system and emerge with more profound hypoglycemia. These symptoms can vary in intensity and presentation depending on the severity of the episode and individual factors.[1][49] Adrenergic symptoms serve as initial alerts and include sweating, tremor, anxiety, palpitations, and hunger. These are mediated by activation of the sympathoadrenal system and commonly appear when blood glucose falls below 70 mg/dL. For instance, patients often report a sense of nervousness or shakiness as the first indicators, prompting recognition and intervention.[49][1][58] Neuroglycopenic symptoms, which indicate brain glucose insufficiency, encompass confusion, dizziness, headache, fatigue, blurred vision, and in severe cases, seizures. These typically develop when glucose levels drop below 55 mg/dL and can impair cognitive function, leading to disorientation or altered mental status. Patients may describe a foggy-headed sensation or visual disturbances that hinder daily activities; this mental fog typically arises after prolonged fasting (e.g., skipping meals), physical exercise, stress, or reactive hypoglycemia (a blood sugar drop 2–4 hours post-meal due to excess insulin release) and clears rapidly after glucose intake.[49][1][48][2][59] Hypoglycemia does not cause skin irritation, itching, or rash. In people with diabetes, such skin issues are typically associated with hyperglycemia (high blood sugar), poor circulation, infections, or reactions to medications, rather than low blood sugar.[2][60] The progression of symptoms often follows a pattern from mild to severe: early episodes are dominated by adrenergic features, providing an opportunity for self-correction through carbohydrate intake, whereas untreated progression shifts toward neuroglycopenic dominance, potentially resulting in loss of hypoglycemia awareness and heightened risk of complications. In severe instances, this can culminate in unconsciousness, with symptoms resolving upon glucose restoration as outlined in Whipple's triad.[49][1][61] Symptom presentation exhibits variability across populations. In the elderly, manifestations are often atypical, including confusion that can be mistaken for dementia or exacerbate existing cognitive decline, resembling stroke-like episodes with focal neurological deficits such as hemiparesis, due to age-related autonomic dysfunction and comorbidities that blunt classic adrenergic responses. Hypoglycemia is particularly dangerous in older adults due to these atypical presentations and associated comorbidities. Among children, symptoms frequently involve behavioral changes like irritability or mood swings rather than overt autonomic signs, complicating timely recognition in pediatric settings.[62][63][61][64]Physical Signs
Hypoglycemia manifests through various observable physical signs during clinical examination, primarily driven by autonomic activation and neuroglycopenic effects from glucose deprivation.[1] Autonomic signs include pallor, resulting from vasoconstriction; diaphoresis, or profuse sweating due to sympathetic stimulation; tachycardia, an elevated heart rate; and hypertension, reflecting catecholamine release.[1][65] These findings are commonly noted in moderate hypoglycemia and can precede more severe neurological changes. Neurological signs encompass altered mental status, ranging from confusion to lethargy; ataxia, indicating impaired coordination; focal neurological deficits that may mimic stroke, such as hemiparesis; and, in extreme cases, progression to coma with loss of consciousness.[1][65] These observations highlight the central nervous system's vulnerability to low glucose levels. Other physical signs may involve hypothermia, particularly in prolonged or severe episodes due to impaired thermoregulation; shallow breathing, often seen in advanced neuroglycopenia; and typically the absence of fever, unless an underlying infection is present.[66][67][65] During examination, priorities include assessing severity using the Glasgow Coma Scale to quantify level of consciousness and evaluating pupil response to light for detecting neurological impairment.[1][65] These tools aid in rapid triage, especially when symptoms like shakiness prompt evaluation.[2]Diagnosis
Clinical Evaluation
The clinical evaluation of suspected hypoglycemia begins with a thorough history and physical examination to establish suspicion based on Whipple's triad—recurrent symptoms consistent with low blood glucose that resolve with its restoration—while identifying potential triggers and risks.[1] This bedside assessment is essential for distinguishing hypoglycemia from other conditions and guiding further investigation.[8] History-taking focuses on the timing of episodes, which may occur in fasting states (e.g., overnight or prolonged abstinence) or postprandially (after meals), helping to differentiate causes such as insulin excess or reactive hypoglycemia.[1] Inquiry into diabetes status is critical, as patients with type 1 or type 2 diabetes are at higher risk, particularly those on insulin therapy or oral agents like sulfonylureas.[68] A detailed review of medications includes insulin dosing, oral antidiabetics, and other drugs that may potentiate hypoglycemia, such as beta-blockers or quinine.[1] Recent dietary intake, including meal composition, timing, and skipping habits, alongside exercise patterns—such as unusual intensity or duration—must be explored, as these can precipitate episodes by altering glucose utilization.[68] Alcohol consumption history is probed, given its inhibitory effect on hepatic gluconeogenesis, often leading to delayed-onset hypoglycemia hours after intake.[1] Risk assessment involves evaluating the frequency and severity of prior episodes, as recurrent events increase the likelihood of underlying pathology.[8] History of hypoglycemic unawareness—where autonomic warning symptoms are absent due to repeated exposure—warrants special attention, as it heightens the danger of severe outcomes.[1] Family history of endocrine disorders, such as insulinomas or other tumors, or genetic conditions affecting glucose regulation, should be elicited to uncover hereditary factors.[68] The physical examination prioritizes vital signs, including blood pressure, heart rate, and temperature, to detect tachycardia, hypotension, or hypothermia indicative of autonomic activation or severe compromise.[1] A neurological assessment is key, screening for neuroglycopenic manifestations such as altered mental status, confusion, focal deficits, seizures, or coma, which reflect brain glucose deprivation.[68] Abdominal palpation is performed to identify masses or tenderness suggestive of insulin-secreting tumors like insulinomas.[8] Red flags that warrant urgent evaluation include a first-time hypoglycemic episode in individuals without a history of diabetes, which requires prompt medical attention to rule out underlying serious conditions such as tumors (e.g., insulinoma) or hormone deficiencies (e.g., adrenal or pituitary insufficiency), as well as recurrent nocturnal hypoglycemia, which may signal an insulinoma or other occult causes requiring urgent evaluation, as these episodes can lead to unrecognized severe events during sleep.[33][1]Laboratory Confirmation
Laboratory confirmation of hypoglycemia begins with the measurement of plasma glucose concentration using a venous blood sample obtained during symptomatic episodes to verify low glucose levels, typically defined as below 55 mg/dL (3.0 mmol/L) in adults without diabetes.[8] This approach aligns with Whipple's triad, requiring documentation of symptoms, low plasma glucose, and resolution upon glucose administration.[53] Point-of-care (POC) glucose testing, while useful for rapid screening, is less accurate than central laboratory methods, particularly in the hypoglycemic range (<70 mg/dL), where discrepancies exceeding 20% from laboratory values occur in up to 57% of cases due to factors such as hematocrit variations, poor perfusion, and device-specific interferences.[69] Laboratory analysis using enzymatic methods (e.g., hexokinase or glucose oxidase) on venous plasma is therefore preferred for definitive confirmation to avoid misdiagnosis.[8] To identify the underlying etiology, a "critical sample" of blood is drawn at the time of hypoglycemia (plasma glucose <50 mg/dL) for measurement of insulin, C-peptide, and beta-hydroxybutyrate levels.[53] Inappropriately elevated insulin (≥3 μU/mL or 18 pmol/L) and C-peptide (≥0.6 ng/mL or 0.2 nmol/L) during hypoglycemia indicate endogenous hyperinsulinism, such as from an insulinoma, while suppressed beta-hydroxybutyrate (≤2.7 mmol/L) supports insulin-mediated suppression of ketogenesis.[8] These markers distinguish hyperinsulinemic causes from other etiologies, like accidental hypoglycemia from exogenous insulin (low C-peptide) or non-insulin-mediated states (elevated beta-hydroxybutyrate).[53] Additional screening for sulfonylureas and insulin antibodies may be included in the critical sample panel.[8] For suspected endogenous hyperinsulinemic hypoglycemia, such as insulinoma, a supervised 72-hour fast is the gold-standard provocative test, conducted in a hospital setting to monitor for hypoglycemia while assessing metabolic responses.[8] The protocol involves baseline venous sampling after an overnight fast, followed by hourly capillary glucose checks (more frequent if <60 mg/dL) and venous blood draws every 6 hours for plasma glucose, insulin, C-peptide, proinsulin, and beta-hydroxybutyrate.[70] The fast terminates upon development of symptoms with plasma glucose <45 mg/dL (2.5 mmol/L), or at 72 hours; a glucagon stimulation test (1 mg IV) is then performed to evaluate hepatic glycogen stores, with a rise >25 mg/dL supporting hyperinsulinism.[8] Incorporation of beta-hydroxybutyrate monitoring allows early termination if levels exceed 2.7 mmol/L (indicating no hyperinsulinism), reducing average fast duration from approximately 58 hours to 50 hours without compromising diagnostic yield.[70] Recent advancements in continuous glucose monitoring (CGM) systems, as emphasized in 2025 guidelines, enhance real-time confirmation of hypoglycemia by providing interstitial glucose trends and alerts for levels <70 mg/dL, particularly beneficial for high-risk patients with recurrent episodes.[5] CGM metrics, such as time below range (<4% for <70 mg/dL and <1% for <54 mg/dL), correlate well with laboratory plasma glucose and have been shown to reduce hypoglycemic events by up to 30% in insulin-treated individuals through predictive algorithms and over-the-counter accessibility approved by the FDA in 2024.[71] While not a replacement for venous sampling during acute confirmation, CGM facilitates ongoing surveillance and etiology assessment in ambulatory settings.[5]Differential Diagnosis
The differential diagnosis of hypoglycemia encompasses various conditions that can produce similar neuroglycopenic or autonomic symptoms, such as sweating, tremors, confusion, and palpitations, necessitating careful evaluation to exclude mimics.[12] A cornerstone of this process is Whipple's triad, which requires documentation of symptoms consistent with hypoglycemia, a plasma glucose level below 55 mg/dL (3.0 mmol/L) during symptoms, and prompt resolution of symptoms following glucose administration; failure to meet all three criteria points away from true hypoglycemia.[12] This triad helps distinguish genuine episodes from pseudohypoglycemia, where symptoms occur but blood glucose remains normal or symptoms do not resolve with glucose correction.[12] Common mimics include anxiety or panic disorders, seizures, and stroke, which can present with overlapping autonomic and neurological features like tachycardia, diaphoresis, dizziness, or altered mental status.[12] In these cases, a key distinction is the persistence of symptoms despite normalization of blood glucose levels, often confirmed through continuous monitoring or response to targeted interventions such as anxiolytics for panic attacks or anticonvulsants for seizures; neuroimaging like CT or MRI may be warranted if focal deficits suggest stroke.[12] Adrenal insufficiency can also mimic hypoglycemia due to cortisol deficiency leading to impaired gluconeogenesis and similar symptoms of fatigue, weakness, and hypotension, but it is differentiated by elevated adrenocorticotropic hormone (ACTH) levels, low cortisol, and response to glucocorticoid replacement rather than glucose alone.[12] Factitious disorder, involving surreptitious administration of insulin or oral hypoglycemics, presents a diagnostic challenge as it induces true hypoglycemia but with atypical laboratory patterns.[72] Distinction relies on measuring insulin, C-peptide, and sulfonylurea levels during hypoglycemia: exogenous insulin shows high insulin with suppressed C-peptide (ratio >1), while sulfonylurea abuse elevates both insulin and C-peptide alongside a positive drug screen, contrasting with endogenous causes like insulinoma where both are inappropriately elevated without exogenous agents.[72] Special considerations include idiopathic postprandial syndrome, where patients experience hypoglycemic-like symptoms 2-5 hours after meals but maintain normal plasma glucose levels (>70 mg/dL), often linked to heightened autonomic sensitivity rather than true reactive hypoglycemia, which requires documented glucose nadir below 55 mg/dL during a mixed meal tolerance test.[73] In cases of reactive hypoglycemia, hemoglobin A1c (HbA1c) levels accurately reflect average glycemia without false elevation or reduction due to episodic lows, as these do not alter red blood cell lifespan or hemoglobin glycation mechanisms akin to anemias or hemoglobin variants. However, high glycemic variability from glucose spikes and dips may limit HbA1c's ability to capture postprandial excursions or symptom severity, making continuous glucose monitoring (CGM) or mixed-meal tests preferable for detailed fluctuation assessment.[74] Alcohol withdrawal represents another overlap, with symptoms like tremors, anxiety, and seizures mimicking hypoglycemia due to autonomic hyperactivity, though it is distinguished by a history of heavy alcohol use, normal or elevated glucose on testing, and improvement with benzodiazepines rather than glucose.[12] The diagnostic approach emphasizes serial laboratory assessments during symptomatic episodes, including glucose, insulin, C-peptide, and beta-hydroxybutyrate, to exclude mimics; if endogenous hyperinsulinism is suspected after ruling out factitious causes, imaging such as CT or MRI of the abdomen may identify pancreatic tumors.[12]Treatment
Acute Management
The acute management of hypoglycemia prioritizes rapid restoration of blood glucose levels to prevent neurological damage, with interventions tailored to the patient's level of consciousness and severity of symptoms.[75] For conscious patients able to swallow, guidelines such as those from Diabetes UK recommend the following steps: test blood glucose if possible to confirm it is low (typically below 4 mmol/L or 70 mg/dL), or treat based on symptoms if unable to test; consume 15-20 g of quick-acting carbohydrate (e.g., 4-5 glucose tablets, 200 ml of a sugary drink like Lucozade, or 5-6 jelly babies); wait 10-15 minutes, then recheck blood glucose; repeat the quick-acting carbohydrate if still below 4 mmol/L; once blood glucose is above 4 mmol/L and symptoms have improved, consume a longer-acting carbohydrate snack (e.g., a sandwich, fruit with crackers, or the next meal if more than 1 hour away).[76] The 10-15 minute wait before rechecking allows time for the ingested carbohydrates to be digested (if complex) and absorbed primarily in the small intestine before entering the bloodstream and significantly raising blood glucose levels. This absorption process typically takes 10-30 minutes or more depending on the carbohydrate type (simple sugars are absorbed more rapidly though not instantaneously, while the presence of fats, proteins, or fiber can slow gastric emptying and delay absorption further), meaning hypoglycemic symptoms may persist briefly even after consumption.[77][78] While carbohydrate sources providing 15-20 grams can treat mild hypoglycemia, combining them with fats, such as cream cheese on half a bagel (which supplies approximately 25-30 grams of carbohydrates), slows gastric emptying and glucose absorption compared to pure simple carbohydrates, making it less ideal for rapid correction but suitable for the follow-up snack to sustain levels and prevent recurrence.[79] Symptoms like shakiness or confusion signal the need for prompt action under this protocol.[80] In cases of severe hypoglycemia where the patient is unconscious, confused, or unable to swallow, intramuscular glucagon is the preferred initial intervention outside hospital settings if available and the caregiver is trained to administer it.[81] The standard dose for adults is 1 mg injected into the upper arm, thigh, or buttocks, which typically raises blood glucose within 10-15 minutes by stimulating hepatic glycogenolysis.[82] Position the person on their side if unconscious, call emergency medical services immediately, and if no response occurs after 15 minutes, a second dose may be given, followed by fast-acting carbohydrates once the patient regains consciousness.[68] Family members or close contacts play a critical role by being trained to recognize severe symptoms and use prescribed glucagon kits, ensuring accessibility and proper storage.[68] Particularly in older adults, severe hypoglycemia is a medical emergency requiring immediate intervention and prompt medical attention to mitigate risks such as prolonged recovery and other complications.[68] For hospitalized patients or those with intravenous access, severe hypoglycemia is treated with an IV bolus of dextrose to achieve rapid correction.[75] A typical adult dose is 25-50 grams of 50% dextrose (D50W), administered as 50-100 mL over 1-3 minutes, though lower concentrations like 10% or 20% dextrose (200 mL or 100 mL, respectively) are preferred in some guidelines to minimize vein irritation and hyperosmolarity risks.[83] Blood glucose should be rechecked every 15-30 minutes post-bolus, with monitoring to avoid rebound hypoglycemia from excessive hyperglycemia triggering endogenous insulin release.[83] Refractory hypoglycemia, often seen in sulfonylurea overdoses or prolonged insulin effects, requires hospital protocols including continuous IV glucose infusion after initial bolus.[81] A 10% dextrose infusion at 100 mL/hour is commonly initiated, with frequent glucose monitoring and adjustments to maintain levels above 70 mg/dL until the underlying cause resolves.[81] In such cases, multidisciplinary input from endocrinologists may be needed to address persistent episodes.[75]Chronic Management
Chronic management of recurrent hypoglycemia in patients with diabetes primarily involves adjusting pharmacotherapy to minimize episodes while maintaining glycemic control. For individuals on insulin therapy, dose reduction of basal or prandial insulin is often the first step, particularly if hypoglycemia occurs frequently despite appropriate lifestyle measures.[5] Switching to ultra-long-acting basal insulins such as insulin degludec can further lower the risk of hypoglycemia compared to intermediate-acting options like NPH or standard glargine, due to its stable pharmacokinetic profile and reduced variability.[84] In patients at high risk, sulfonylureas and meglitinides should be avoided or discontinued, as these agents carry a substantial hypoglycemia risk without the flexibility of insulin adjustments.[5] Lifestyle modifications play a central role in preventing recurrent episodes. Patients are advised to consume frequent, balanced meals and snacks to maintain steady blood glucose levels, avoiding prolonged fasting or skipped meals that can precipitate hypoglycemia.[85] Carbohydrate counting is essential for those on insulin, allowing precise matching of insulin doses to carbohydrate intake and reducing the likelihood of mismatches that lead to lows.[86] Exercise planning is equally important; physical activity should be scheduled with pre- and post-exercise carbohydrate intake to counteract glucose utilization, and patients are encouraged to monitor glucose before, during, and after sessions.[87] Ongoing monitoring is critical for hypoglycemia-prone individuals. Self-monitoring of blood glucose (SMBG) should occur at least 4-10 times daily, including before meals, at bedtime, and during suspected episodes, with increased frequency as needed to detect patterns and adjust therapy.[88] For those with recurrent hypoglycemia, HbA1c targets may be relaxed to greater than 7.5% to prioritize avoidance of severe events over strict glycemic control.[5] Glucagon kits should be kept accessible as a backup for severe episodes.[5] In non-diabetic causes of recurrent hypoglycemia, management targets the underlying etiology. For insulinoma, octreotide, a somatostatin analog, is used to suppress insulin secretion and control symptoms in approximately 50% of cases, often as a bridge to surgery.[89] In congenital hyperinsulinism, diazoxide is the first-line medical therapy, administered at doses of 5-15 mg/kg/day to inhibit insulin release and maintain euglycemia in responsive patients.[90]Emerging Therapies
Recent advancements in hypoglycemia management emphasize technologies and pharmacotherapies that minimize severe episodes while improving glycemic control, particularly in patients with type 1 diabetes (T1D) and type 2 diabetes (T2D). Continuous glucose monitoring (CGM) integrated with hybrid closed-loop (HCL) systems represents a key innovation, automating insulin delivery to prevent lows. According to the American Diabetes Association's 2025 Standards of Care, these automated insulin delivery systems, including HCL, effectively reduce hypoglycemia risk in insulin-treated individuals by suspending or adjusting insulin based on real-time glucose trends.[5] In T1D, HCL systems have demonstrated reductions in hypoglycemia compared to sensor-augmented pumps, with real-world data from 2025 studies confirming that HCL achieves time in range above 70% while lowering hypoglycemic coma rates to 0.62 per 100 patient-years.[91] Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are being investigated as low-hypoglycemia-risk adjuncts, especially for post-bariatric hypoglycemia (PBH), where rapid postprandial glucose fluctuations pose challenges. These agents slow gastric emptying and enhance insulin secretion in a glucose-dependent manner, potentially reducing PBH episodes without increasing severe lows. A 2025 systematic review of pharmacological therapies for PBH found that evidence for GLP-1 RAs like liraglutide remains inconsistent and is primarily derived from case reports and small studies.[92] Case reports from 2025 have reported symptomatic improvement in some patients with PBH treated with liraglutide, alongside weight stabilization.[93] Other options like acarbose and calcium channel blockers also show limited, inconsistent evidence in the same review. Investigational therapies, such as the GLP-1 receptor antagonist avexitide, are in phase 3 trials for PBH as of 2025.[39] Semaglutide has shown potential benefits in similar contexts, positioning GLP-1 RAs as options for this subgroup due to their dual role in glycemic and weight control, pending further evidence.[92] Fixed-ratio combinations like iDegLira (insulin degludec/liraglutide) offer improved outcomes over traditional regimens, particularly in T2D patients transitioning from premixed insulins. This therapy combines basal insulin with GLP-1 RA action, enhancing time in range while minimizing hypoglycemia. A 2025 continuous glucose monitoring study switching patients from premixed insulin to iDegLira reported fewer hypoglycemic events (rate ratio 0.65) and a 1.2% HbA1c reduction without weight gain.[94] Compared to premixed insulin, iDegLira achieved superior glycemic control with 30-40% lower hypoglycemia incidence in real-world 2025 analyses, attributed to its glucose-dependent effects.[94] These findings align with broader 2025 meta-analyses confirming iDegLira's safety profile, including reduced severe hypo risk versus multiple daily injections.[95] Among other innovations, nasal glucagon sprays provide rapid, needle-free rescue for severe hypoglycemia, addressing barriers to traditional injectable forms. Baqsimi (glucagon nasal powder), approved for expansion in 2025 to patients aged 1 year and older, raises blood glucose within 15 minutes by stimulating hepatic glycogenolysis.[96] Clinical simulations in 2025 demonstrated faster administration and fewer errors with nasal delivery versus injections, improving emergency response in community settings.[97] Similarly, sodium-glucose cotransporter-2 (SGLT2) inhibitors exhibit hypo-sparing effects in T2D, lowering severe hypoglycemia risk by 20-30% when added to insulin regimens due to their insulin-independent mechanism. The 2025 ADA guidelines highlight SGLT2 inhibitors' role in reducing hypo events alongside cardiovascular benefits in T2D.[84]Prevention
Strategies for Diabetics
Education on recognizing and managing hypoglycemia is a cornerstone of prevention for diabetic patients, particularly those using insulin or sulfonylureas. Structured programs emphasize symptom identification, such as shakiness, sweating, and confusion, and train individuals to respond promptly with the 15-15 rule—consuming 15 grams of fast-acting carbohydrates and rechecking blood glucose after 15 minutes.[5] Sick-day rules instruct patients to monitor blood glucose more frequently during illness, adjust insulin doses to avoid lows while preventing dehydration, and continue carbohydrate intake to maintain stable levels, as illness can unpredictably alter glucose metabolism.[98] All patients at risk should receive education on glucagon administration, with nasal or injectable forms prescribed for severe episodes, and caregivers trained to use them effectively.[5] Technological interventions play a key role in preempting hypoglycemia. Continuous glucose monitoring (CGM) systems with customizable alerts notify users of impending lows, enabling proactive carbohydrate intake or insulin adjustments, and are recommended for those with frequent or severe events.[5] Automated insulin delivery systems, such as hybrid closed-loop pumps, automatically suspend or reduce insulin delivery when glucose approaches low thresholds, significantly lowering hypoglycemia incidence in type 1 diabetes.[5] Insulin regimens should prioritize flexibility to mitigate risk. Providers routinely reassess dosing after any level 2 (glucose <54 mg/dL) or level 3 (severe) hypoglycemia, often simplifying or deintensifying therapy—such as reducing basal insulin or switching agents—to prevent recurrence while maintaining glycemic control.[5] To avoid hypoglycemia-associated autonomic failure (HAAF), which blunts counter-regulatory responses and awareness after recurrent lows, strategies focus on scrupulous avoidance of antecedent hypoglycemia through conservative targets and education; for those with impaired awareness, evidence-based training programs involving controlled mild hypos can partially restore symptom recognition.[52] Regular monitoring underpins these efforts. Self-monitoring of blood glucose (SMBG) is advised at least before meals and bedtime for insulin users, with increased frequency—up to every 2-4 hours—during high-risk periods like exercise or illness to detect and avert lows early.[99] Nocturnal monitoring is particularly critical, as asymptomatic nighttime hypos affect up to 50% of type 1 patients; CGM facilitates this by tracking overnight trends without awakening.[5] Glycemic goals, such as an A1C below 7%, should be individualized to minimize hypoglycemia risk, with less stringent targets (e.g., <8%) for older adults or those with comorbidities where hypo unawareness heightens danger.[5]Strategies for Non-Diabetics
For individuals without diabetes, preventing hypoglycemia involves addressing underlying causes through targeted lifestyle adjustments and medical interventions, as episodes often stem from sporadic or organic factors rather than chronic glucose dysregulation.[28] Key strategies emphasize maintaining stable blood glucose levels via dietary patterns and avoiding triggers, while cause-specific measures focus on high-risk scenarios such as metabolic disorders or surgical procedures.[33] Lifestyle modifications form the cornerstone of prevention, particularly for reactive hypoglycemia, which occurs postprandially in non-diabetics due to exaggerated insulin responses. Consuming small, frequent meals every 3-4 hours—incorporating complex carbohydrates, proteins, and healthy fats—helps sustain glucose levels and prevents rapid drops.[59] Avoiding prolonged fasting, excessive alcohol intake, and high-glycemic-index foods like sugary items or refined carbohydrates is essential, as these can provoke insulin surges and subsequent hypoglycemia.[100] Limiting caffeine may also reduce symptomatic episodes by minimizing counterregulatory hormone fluctuations.[101] Cause-specific strategies target identifiable etiologies to mitigate risks. For inborn errors of metabolism, such as congenital hyperinsulinism or glycogen storage diseases, genetic counseling is recommended to inform family planning and enable early dietary interventions, like fructose avoidance in hereditary fructose intolerance.[33] In preparation for bariatric surgery, preoperative screening—including oral glucose tolerance testing (OGTT) and history assessment for prior hypoglycemia—identifies at-risk patients, as lower 120-minute OGTT glucose levels predict post-bariatric hyperinsulinemic hypoglycemia.[102] Hormone replacement therapy prevents episodes in endocrine deficiencies; for instance, hydrocortisone for adrenal insufficiency in Addison's disease restores cortisol levels to support gluconeogenesis.[33] Neonatal hypoglycemia prevention prioritizes at-risk infants through maternal and immediate postnatal measures. Optimal maternal glucose control during pregnancy reduces fetal hyperinsulinism in vulnerable cases, while early enteral feeding—via breast milk or formula within the first hour of life—promotes stable glucose in infants prone to transient lows due to immaturity or perinatal stress.[103][104] General preventive actions include avoiding medications known to induce hypoglycemia and monitoring for tumors. Discontinuing or avoiding drugs like quinine, which stimulates insulin release and can cause symptomatic lows especially in renal impairment, is advised for those with leg cramps or malaria risk.[105] For insulinomas or non-islet cell tumors, regular surveillance via imaging (e.g., CT or MRI) enables timely surgical resection to prevent recurrent fasting hypoglycemia.[28]Complications and Prognosis
Acute Complications
Severe hypoglycemia, if left untreated, can rapidly progress from initial symptoms such as confusion and sweating to life-threatening acute complications, primarily due to neuroglycopenia and counter-regulatory hormonal responses.[1][106] Neurological effects are among the most immediate dangers, with profound glucose deprivation leading to seizures, coma, and potential brain injury through energy failure and neuronal damage akin to hypoxic insult.[107][1] Prolonged neuroglycopenia impairs cerebral metabolism, causing selective vulnerability in brain regions like the hippocampus and cortex, which can result in irreversible damage if glucose levels remain critically low.[108][109] Cardiovascular complications arise from autonomic activation and direct electrophysiological changes, including cardiac arrhythmias and QT interval prolongation, which heighten the risk of sudden death.[110][111] Hypoglycemia-induced QT prolongation, observed in both diabetic and non-diabetic individuals, predisposes to ventricular arrhythmias like torsades de pointes.[112][113] In severe cases, mortality rates attributed to these events range from 4% to 10% among affected patients, particularly those with type 1 diabetes.[114][48] In ambulatory patients, altered mental status and motor impairment during hypoglycemic episodes increase the likelihood of falls and accidents, often resulting in traumatic injuries such as fractures or head trauma.[115][116] Studies indicate that severe hypoglycemia is associated with a 70% greater risk of falls in older adults with diabetes, contributing to emergency visits and further complications.[117] Older adults are particularly vulnerable to severe hypoglycemia, with heightened risks of cardiovascular events such as arrhythmias and acute coronary syndromes triggered by autonomic activation and catecholamine surges, as well as potentially slower recovery from episodes due to comorbidities and reduced physiological reserves.[110][111] Following an episode of severe hypoglycemia, especially if overcorrected with glucose administration, rebound hyperglycemia may occur via the Somogyi effect, where counter-regulatory hormones like glucagon and cortisol drive excessive glucose release, potentially complicating glycemic control.[118]Long-Term Effects
Recurrent hypoglycemia in individuals with diabetes has been linked to progressive neurological impairments, including cognitive decline and memory deficits. Studies indicate that repeated severe episodes can cause histopathological changes in the brain, leading to memory impairments and overall cognitive dysfunction. Furthermore, 2024 research highlights that recurrent hypoglycemia augments the risk of dementia in patients with type 2 diabetes, potentially through mechanisms involving excitotoxicity and synaptic dysfunction that mimic Alzheimer's disease pathology.[119] A 2025 analysis further supports that such episodes impair cognitive reserve over time, accelerating neurodegeneration and elevating dementia risk.[120] On the cardiovascular front, recurrent hypoglycemia contributes to increased mortality and arrhythmic events due to repeated physiological stress. Hypoglycemic episodes are associated with a heightened rate of cardiac arrhythmias, even in non-diabetic individuals, through dysregulation of ion channels and catecholamine surges. Clinical data from 2025 reveal that severe hypoglycemia elevates the risk of adverse cardiovascular complications, with mortality rates following such events estimated at 2-4% in diabetic patients, reflecting a broader increase in all-cause and cardiovascular death.[121] In neonates, severe or recurrent hypoglycemia poses significant developmental risks, particularly when blood glucose falls below 36 mg/dL. According to 2025 NIH-funded studies, such episodes are tied to neurological injury, resulting in long-term developmental delays, reduced IQ, and impairments in motor and mental development.[122] These outcomes underscore the vulnerability of the immature brain to glucose deprivation, with persistent effects on cognitive and behavioral trajectories. Beyond these domain-specific impacts, recurrent hypoglycemia promotes the progression to impaired awareness of hypoglycemia (IAH), diminishes quality of life, and induces brain metabolic inflexibility. Repeated exposures trigger adaptive central nervous system changes that blunt symptom perception, fostering IAH and escalating severe event frequency. This cycle correlates with reduced quality of life due to heightened fear of hypoglycemia and daily management burdens. Additionally, 2024-2025 evidence points to impaired neuronal energy metabolism, limiting the brain's ability to adapt fuel sources during low glucose states and contributing to sustained cognitive vulnerabilities.[120]History and Etymology
Historical Development
The understanding of hypoglycemia began in the mid-19th century with foundational work on glucose homeostasis. French physiologist Claude Bernard discovered the glycogenic function of the liver in 1855, revealing that the organ stores glycogen and releases glucose to maintain blood sugar levels during fasting, which provided early insights into disruptions like low blood glucose.[123] This work illuminated the pathways of gluconeogenesis and carbohydrate metabolism, setting the stage for later recognition of hypoglycemic states.[124] The clinical recognition of hypoglycemia emerged prominently in the early 20th century following the discovery of insulin. In 1921, Frederick Banting and Charles Best isolated insulin from canine pancreases, revolutionizing diabetes treatment but introducing hypoglycemia as a common complication of insulin therapy due to excessive dosing or inadequate carbohydrate intake.[125] Pioneering diabetologist Elliott P. Joslin, who observed the transformative effects of insulin in 1922, emphasized the risks of recurrent hypoglycemia in his writings in the 1920s. Key diagnostic milestones advanced in the 1930s with Allen Whipple's formulation of the "Whipple's triad" in 1938, which established criteria for insulinoma-related hypoglycemia: symptoms consistent with low blood glucose, documented plasma glucose below 50 mg/dL during symptoms, and rapid resolution upon glucose administration.[1] The 1970s saw significant progress in elucidating counter-regulatory mechanisms, with Philip E. Cryer's research demonstrating how hormones like glucagon, epinephrine, cortisol, and growth hormone respond to falling glucose levels to prevent or correct hypoglycemia, highlighting defects in diabetes that impair these defenses.[126] The advent of continuous glucose monitoring (CGM) in the early 2000s marked a technological milestone in hypoglycemia management. The first FDA-approved CGM device, the MiniMed Continuous Glucose Monitoring System, became available in 1999 for retrospective data analysis, evolving by the mid-2000s to real-time monitoring with alarms for impending lows, reducing severe hypoglycemic events in type 1 diabetes patients.[127] In the 2020s, focus shifted toward hypoglycemia unawareness, with the American Diabetes Association's 2025 Standards of Care recommending individualized glycemic targets, CGM use for early detection, and education to restore awareness in at-risk individuals through strategies like antecedent hypo avoidance.[5]Etymology
The term "hypoglycemia" originates from Ancient Greek roots: the prefix hypo- meaning "under" or "below," glykys meaning "sweet," and the suffix -emia denoting a blood condition, collectively translating to "low sweet blood" or a deficiency of sugar in the blood.[128][129] This neologism was first recorded in medical literature in the late 19th century, specifically around 1893 in its Latinized form, predating widespread clinical recognition of the condition.[128][130] Following the discovery of insulin in 1921 by Frederick Banting and colleagues, which enabled treatments for diabetes but also revealed risks of induced low blood glucose, the term "hypoglycemia" entered broader medical usage to describe these episodes.[131] In the 1920s and 1930s, alternative phrasing like "hyperinsulinism"—proposed by Seale Harris in 1924 to account for spontaneous cases without overt insulin excess—gained traction as an explanatory framework, though "hypoglycemia" increasingly became the standard descriptor for the state itself.[132][133] In the 1960s, the term "neuroglycopenia" was introduced by Vincent Marks and colleagues, specifically denoting the brain-specific symptoms arising from glucose deprivation during hypoglycemia.[134] Modern standardization occurred through guidelines from the American Diabetes Association, notably a 2005 workgroup report that classified hypoglycemia by severity levels (e.g., biochemical, symptomatic, severe) to improve reporting and management in diabetes care.[6] Subsequent updates, such as the 2018 international consensus, further refined these definitions for regulatory and clinical consistency.[135]References
- https://en.wiktionary.org/wiki/hypoglycemia