

Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Lesser trochanter
View on Wikipedia| Lesser trochanter | |
|---|---|
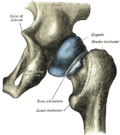
 Left hip-joint, opened by removing the floor of the acetabulum from within the pelvis. | |
 Upper extremity of right femur viewed from behind and above. | |
| Details | |
| Insertions | Psoas major, iliacus |
| Identifiers | |
| Latin | trochanter minor |
| TA98 | A02.5.04.007 |
| TA2 | 1366 |
| FMA | 32853 |
| Anatomical terms of bone | |
In human anatomy, the lesser trochanter is a conical, posteromedial, bony projection from the shaft of the femur. It serves as the principal insertion site of the iliopsoas muscle.[1]
Structure
[edit]The lesser trochanter is a conical posteromedial projection of the shaft of the femur, projecting from the posteroinferior aspect of its junction with the femoral neck.[1]
The summit and anterior surface of the lesser trochanter are rough, whereas its posterior surface is smooth.[1]
From its apex three well-marked borders extend:[2]
- two of these are above
- a medial continuous with the lower border of the femur neck
- a lateral with the intertrochanteric crest
- the inferior border is continuous with the middle division of the linea aspera
Attachments
[edit]The summit of the lesser trochanter gives insertion to the tendon of the psoas major muscle and the iliacus muscle;[3] the lesser trochanter represents the principal attachment of the iliopsoas.[1]
Anatomical relations
[edit]The intertrochanteric crest (which demarcates the junction of the femoral shaft and neck posteriorly) extends between the lesser trochanter and the greater trochanter on the posterior surface of the femur.[1]
Clinical significance
[edit]
The lesser trochanter can be involved in an avulsion fracture.[4]
Other animals
[edit]Paleontology
[edit]The position of the lesser trochanter close to the head of the femur is one of the defining characteristics of the Prozostrodontia, which is the clade of cynodonts including mammals and their closest non-mammaliform relatives. It was erected as a node-based taxon as the least inclusive clade containing Prozostrodon brasiliensis, Tritylodon langaevus, Pachygenelus monus, and Mus musculus (the house mouse).[5]
All living mammals have a lesser trochanter, whose size, shape, and position is distinctive to their species.
Additional images
[edit]This gallery of anatomic features needs cleanup to abide by the medical manual of style. |
-
 Right femur. Posterior surface.
Right femur. Posterior surface. -
 Right hip-joint from the front.
Right hip-joint from the front. -
 Capsule of hip-joint (distended). Posterior aspect.
Capsule of hip-joint (distended). Posterior aspect. -
 Hip joint. Lateral view. Lesser trochanter
Hip joint. Lateral view. Lesser trochanter -
 Muscles of thigh. Anterior views.
Muscles of thigh. Anterior views.




See also
[edit]References
[edit]![]() This article incorporates text in the public domain from page 245 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 245 of the 20th edition of Gray's Anatomy (1918)
- ^ a b c d e Gray's anatomy : the anatomical basis of clinical practice. Susan Standring (Forty-second ed.). [New York]. 2021. p. 1362. ISBN 978-0-7020-7707-4. OCLC 1201341621.
{{cite book}}: CS1 maint: location missing publisher (link) CS1 maint: others (link) - ^ Gray, Henry (1918). Gray's Anatomy (20th ed.). p. 245.
- ^ Federle, Michael P.; Rosado-de-Christenson, Melissa L.; Raman, Siva P.; Carter, Brett W., eds. (2017-01-01), "Female Pelvic Floor", Imaging Anatomy: Chest, Abdomen, Pelvis (Second Edition), Elsevier, pp. 1050–1077, ISBN 978-0-323-47781-9, retrieved 2021-01-22
{{citation}}: CS1 maint: work parameter with ISBN (link) - ^ Khoury JG, Brandser EA, Found EM, Buckwalter JA (1998). "Non-traumatic lesser trochanter avulsion: a report of three cases". Iowa Orthop J. 18: 150–4. PMC 2378165. PMID 9807723.
- ^ Liu, J.; Olsen, P. (2010). "The Phylogenetic Relationships of Eucynodontia (Amniota: Synapsida)". Journal of Mammalian Evolution. 17 (3): 151. doi:10.1007/s10914-010-9136-8. S2CID 40871206.
External links
[edit]- Anatomy figure: 13:01-11 at Human Anatomy Online, SUNY Downstate Medical Center
- lljoints at The Anatomy Lesson by Wesley Norman (Georgetown University) (hipjointanterior, hipjointposterior)
{kind=link}
{kind=link}