Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Talus bone
The talus (/ˈteɪləs/; Latin for ankle or ankle bone; pl.: tali), talus bone, astragalus (/əˈstræɡələs/), or ankle bone is one of the group of foot bones known as the tarsus. The tarsus forms the lower part of the ankle joint. It transmits the entire weight of the body from the lower legs to the foot.
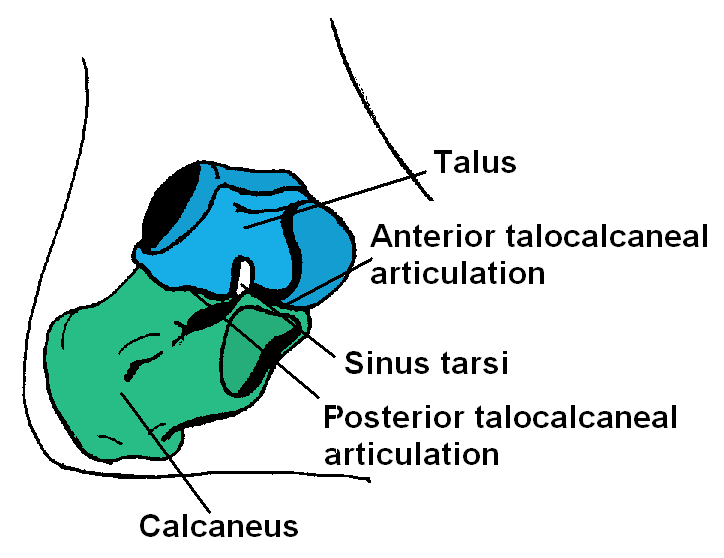
The talus has joints with the two bones of the lower leg, the tibia and thinner fibula. These leg bones have two prominences (the lateral and medial malleoli) that articulate with the talus. At the foot end, within the tarsus, the talus articulates with the calcaneus (heel bone) below, and with the curved navicular bone in front; together, these foot articulations form the ball-and-socket-shaped talocalcaneonavicular joint.
The talus is the second largest of the tarsal bones; it is also one of the bones in the human body with the highest percentage of its surface area covered by articular cartilage. It is also unusual in that it has a retrograde blood supply, i.e. arterial blood enters the bone at the distal end.[citation needed]
In humans, no muscles attach to the talus, unlike most bones, and its position therefore depends on the position of the neighbouring bones.
Though irregular in shape, the talus can be subdivided into three parts.
Facing anteriorly, the head carries the articulate surface of the navicular bone, and the neck, the roughened area between the body and the head, has small vascular channels.
The body features several prominent articulate surfaces: On its superior side is the trochlea tali, which is semi-cylindrical, and it is flanked by the articulate facets for the two malleoli. The ankle mortise, the fork-like structure of the malleoli, holds these three articulate surfaces in a steady grip, which guarantees the stability of the ankle joint. However, because the trochlea is wider in front than at the back (approximately 5–6 mm) the stability in the joint vary with the position of the foot: with the foot dorsiflexed (toes pulled upward) the ligaments of the joint are kept stretched, which guarantees the stability of the joint; but with the foot plantarflexed (as when standing on the toes) the narrower width of the trochlea causes the stability to decrease. Behind the trochlea is a posterior process with a medial and a lateral tubercle separated by a groove for the tendon of the flexor hallucis longus. Exceptionally, the lateral of these tubercles forms an independent bone called os trigonum or accessory talus; it may represent the tarsale proximale intermedium. On the bone's inferior side, three articular surfaces serve for the articulation with the calcaneus, and several variously developed articular surfaces exist for the articulation with ligaments.
For descriptive purposes the talus bone is divided into three sections, neck, body, and head.
Hub AI
Talus bone AI simulator
(@Talus bone_simulator)
Talus bone
The talus (/ˈteɪləs/; Latin for ankle or ankle bone; pl.: tali), talus bone, astragalus (/əˈstræɡələs/), or ankle bone is one of the group of foot bones known as the tarsus. The tarsus forms the lower part of the ankle joint. It transmits the entire weight of the body from the lower legs to the foot.
The talus has joints with the two bones of the lower leg, the tibia and thinner fibula. These leg bones have two prominences (the lateral and medial malleoli) that articulate with the talus. At the foot end, within the tarsus, the talus articulates with the calcaneus (heel bone) below, and with the curved navicular bone in front; together, these foot articulations form the ball-and-socket-shaped talocalcaneonavicular joint.
The talus is the second largest of the tarsal bones; it is also one of the bones in the human body with the highest percentage of its surface area covered by articular cartilage. It is also unusual in that it has a retrograde blood supply, i.e. arterial blood enters the bone at the distal end.[citation needed]
In humans, no muscles attach to the talus, unlike most bones, and its position therefore depends on the position of the neighbouring bones.
Though irregular in shape, the talus can be subdivided into three parts.
Facing anteriorly, the head carries the articulate surface of the navicular bone, and the neck, the roughened area between the body and the head, has small vascular channels.
The body features several prominent articulate surfaces: On its superior side is the trochlea tali, which is semi-cylindrical, and it is flanked by the articulate facets for the two malleoli. The ankle mortise, the fork-like structure of the malleoli, holds these three articulate surfaces in a steady grip, which guarantees the stability of the ankle joint. However, because the trochlea is wider in front than at the back (approximately 5–6 mm) the stability in the joint vary with the position of the foot: with the foot dorsiflexed (toes pulled upward) the ligaments of the joint are kept stretched, which guarantees the stability of the joint; but with the foot plantarflexed (as when standing on the toes) the narrower width of the trochlea causes the stability to decrease. Behind the trochlea is a posterior process with a medial and a lateral tubercle separated by a groove for the tendon of the flexor hallucis longus. Exceptionally, the lateral of these tubercles forms an independent bone called os trigonum or accessory talus; it may represent the tarsale proximale intermedium. On the bone's inferior side, three articular surfaces serve for the articulation with the calcaneus, and several variously developed articular surfaces exist for the articulation with ligaments.
For descriptive purposes the talus bone is divided into three sections, neck, body, and head.