_chest_radiograph_(X-ray).jpg/250px-Normal_posteroanterior_(PA)_chest_radiograph_(X-ray).jpg "Chest radiograph")
_chest_radiograph_(X-ray).jpg/1748px-Normal_posteroanterior_(PA)_chest_radiograph_(X-ray).jpg)
Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Chest radiograph
View on Wikipedia| Chest radiograph | |
|---|---|
_chest_radiograph_(X-ray).jpg) A normal posteroanterior (PA) chest radiograph of someone without any signs of injury. Dx and Sin stand for "right" and "left" respectively. | |
| Specialty | Radiology |
| ICD-9-CM | 87.3-87.4 |
| MeSH | D013902 |
| MedlinePlus | 003804 |
A chest radiograph, chest X-ray (CXR), or chest film is a projection radiograph of the chest used to diagnose conditions affecting the chest, its contents, and nearby structures. Chest radiographs are the most common film taken in medicine.
Like all methods of radiography, chest radiography employs ionizing radiation in the form of X-rays to generate images of the chest. The mean radiation dose to an adult from a chest radiograph is around 0.02 mSv (2 mrem) for a front view (PA, or posteroanterior) and 0.08 mSv (8 mrem) for a side view (LL, or latero-lateral).[1] Together, this corresponds to a background radiation equivalent time of about 10 days.[2]
Medical uses
[edit]
Conditions commonly identified by chest radiography
- Pneumonia
- Pneumothorax
- Interstitial lung disease
- Heart failure
- Bone fracture
- Hiatal hernia
- Pulmonary tuberculosis
Chest radiographs are used to diagnose many conditions involving the chest wall, including its bones, and also structures contained within the thoracic cavity including the lungs, heart, and great vessels. Pneumonia and congestive heart failure are very commonly diagnosed by chest radiograph. Chest radiographs are also used to screen for job-related lung disease in industries such as mining where workers are exposed to dust.[3]
For some conditions of the chest, radiography is good for screening but poor for diagnosis. When a condition is suspected based on chest radiography, additional imaging of the chest can be obtained to definitively diagnose the condition or to provide evidence in favor of the diagnosis suggested by initial chest radiography. Unless a fractured rib is suspected of being displaced, and therefore likely to cause damage to the lungs and other tissue structures, x-ray of the chest is not necessary as it will not alter patient management.
The main regions where a chest X-ray may identify problems may be summarized as ABCDEF by their first letters:[4]
- Airways, including hilar adenopathy or enlargement
- Breast shadows
- Bones, e.g. rib fractures and lytic bone lesions
- Cardiac silhouette, detecting cardiac enlargement
- Costophrenic angles, including pleural effusions
- Diaphragm, e.g. evidence of free air, indicative of perforation of an abdominal viscus
- Edges, e.g. apices for fibrosis, pneumothorax, pleural thickening or plaques
- Extrathoracic tissues
- Fields (lung parenchyma), being evidence of alveolar flooding
- Failure, e.g. alveolar air space disease with prominent vascularity with or without pleural effusions
Views
[edit]
.jpg)
Different views (also known as projections) of the chest can be obtained by changing the relative orientation of the body and the direction of the x-ray beam. The most common views are posteroanterior, anteroposterior, and lateral. In a posteroanterior (PA) view, the x-ray source is positioned so that the x-ray beam enters through the posterior (back) aspect of the chest and exits out of the anterior (front) aspect, where the beam is detected. To obtain this view, the patient stands facing a flat surface behind which is an x-ray detector. A radiation source is positioned behind the patient at a standard distance (most often 6 feet, 1,8m), and the x-ray beam is fired toward the patient.
In anteroposterior (AP) views, the positions of the x-ray source and detector are reversed: the x-ray beam enters through the anterior aspect and exits through the posterior aspect of the chest. AP chest x-rays are harder to read than PA x-rays [citation needed] and are therefore generally reserved for situations where it is difficult for the patient to get an ordinary chest x-ray, such as when the patient is bedridden. In this situation, mobile X-ray equipment is used to obtain a lying down chest x-ray (known as a "supine film"). As a result, most supine films are also AP.
Lateral views of the chest are obtained in a similar fashion as the posteroanterior views, except in the lateral view, the patient stands with both arms raised and the left side of the chest pressed against a flat surface.
Typical views
[edit]Required projections can vary by country and hospital, although an erect posteroanterior (PA) projection is typically the first preference. If this is not possible, then an anteroposterior view will be taken. Further imaging depends on local protocols which is dependent on the hospital protocols, the availability of other imaging modalities and the preference of the image interpreter. In the UK, the standard chest radiography protocol is to take an erect posteroanterior view only and a lateral one only on request by a radiologist.[5] In the US, chest radiography includes a PA and Lateral with the patient standing or sitting up. Special projections include an AP in cases where the image needs to be obtained stat (immediately) and with a portable device, particularly when a patient cannot be safely positioned upright. Lateral decubitus may be used for visualization of air-fluid levels if an upright image cannot be obtained. Anteroposterior (AP) Axial Lordotic projects the clavicles above the lung fields, allowing better visualization of the apices (which is extremely useful when looking for evidence of primary tuberculosis).
Additional views
[edit]- Decubitus – taken while the patient is lying down, typically on their side. Useful for differentiating pleural effusions from consolidation (e.g. pneumonia) and loculated effusions from free fluid in the pleural space. In effusions, the fluid layers out (by comparison to an up-right view, when it often accumulates in the costophrenic angles).
- Lordotic view – used to visualize the apex of the lung, to pick up abnormalities such as a Pancoast tumor.
- Expiratory view – helpful for the diagnosis of pneumothorax.
- Oblique view – useful for the visualization of the ribs and sternum. Although it is necessary to do the appropriate adaptations to the x-ray dosage to be used.
Landmarks
[edit]

In the average person, the diaphragm should be intersected by the 5th to 7th anterior ribs at the mid-clavicular line, and 9 to 10 posterior ribs should be viewable on a normal PA inspiratory film. An increase in the number of viewable ribs implies hyperinflation, as can occur, for example, with obstructive lung disease or foreign body aspiration. A decrease implies hypoventilation, as can occur with restrictive lung disease, pleural effusions or atelectasis. Underexpansion can also cause interstitial markings due to parenchymal crowding, which can mimic the appearance of interstitial lung disease. Enlargement of the right descending pulmonary artery can indirectly reflect changes of pulmonary hypertension, with a size greater than 16 mm abnormal in men and 15 mm in women.[6]
Appropriate penetration of the film can be assessed by faint visualization of the thoracic spines and lung markings behind the heart. The right diaphragm is usually higher than the left, with the liver being situated beneath it in the abdomen. The minor fissure can sometimes be seen on the right as a thin horizontal line at the level of the fifth or sixth rib. Splaying of the carina can also suggest a tumor or process in the middle mediastinum or enlargement of the left atrium, with a normal angle of approximately 60 degrees. The right paratracheal stripe is also important to assess, as it can reflect a process in the posterior mediastinum, in particular the spine or paraspinal soft tissues; normally it should measure 3 mm or less. The left paratracheal stripe is more variable and only seen in 25% of normal patients on posteroanterior views.[7]
Localization of lesions or inflammatory and infectious processes can be difficult to discern on chest radiograph, but can be inferred by silhouetting and the hilum overlay sign with adjacent structures. If either hemidiaphragm is blurred, for example, this suggests the lesion to be from the corresponding lower lobe. If the right heart border is blurred, than the pathology is likely in the right middle lobe, though a cavum deformity can also blur the right heard border due to indentation of the adjacent sternum. If the left heart border is blurred, this implies a process at the lingula.[8]
Abnormalities
[edit]Nodule
[edit]A lung nodule is a discrete opacity in the lung which may be caused by:
- Neoplasm: benign or malignant
- Granuloma: tuberculosis
- Infection: round pneumonia
- Vascular: infarct, varix, granulomatosis with polyangiitis, rheumatoid arthritis
There are a number of features that are helpful in suggesting the diagnosis:
- rate of growth
- Doubling time of less than one month: sarcoma/infection/infarction/vascular
- Doubling time of six to 18 months: benign tumor/malignant granuloma
- Doubling time of more than 24 months: benign nodule neoplasm
- calcification
- margin
- smooth
- lobulated
- presence of a corona radiata
- shape
- site
If the nodules are multiple, the differential is then smaller:
- infection: tuberculosis, fungal infection, septic emboli
- neoplasm: e.g., metastases, lymphoma, hamartoma
- sarcoidosis
- alveolitis
- auto-immune disease: e.g., granulomatosis with polyangiitis, rheumatoid arthritis
- inhalation (e.g., pneumoconiosis)
Cavities
[edit]A cavity is a walled hollow structure within the lungs. Diagnosis is aided by noting:
- wall thickness
- wall outline
- changes in the surrounding lung
The causes include:
- cancer
- infarct (usually from a pulmonary embolus)
- infection: e.g., Staphylococcus aureus, tuberculosis, Gram negative bacteria (especially Klebsiella pneumoniae), anaerobic bacteria, and fungus
- Granulomatosis with polyangiitis
Pleural abnormalities
[edit]Fluid in space between the lung and the chest wall is termed a pleural effusion. There needs to be at least 75 mL of pleural fluid in order to blunt the costophrenic angle on the lateral chest radiograph and 200 mL of pleural fluid in order to blunt the costophrenic angle on the posteroanterior chest radiograph. On a lateral decubitus, amounts as small as 50ml of fluid are possible. Pleural effusions typically have a meniscus visible on an erect chest radiograph, but loculated effusions (as occur with an empyema) may have a lenticular shape (the fluid making an obtuse angle with the chest wall).
Pleural thickening may cause blunting of the costophrenic angle, but is distinguished from pleural fluid by the fact that it occurs as a linear shadow ascending vertically and clinging to the ribs.
Diffuse shadowing
[edit]The differential for diffuse shadowing is very broad and can defeat even the most experienced radiologist. It is seldom possible to reach a diagnosis on the basis of the chest radiograph alone: high-resolution CT of the chest is usually required and sometimes a lung biopsy. The following features should be noted:
- type of shadowing (lines, dots or rings)
- reticular (crisscrossing lines)
- companion shadow (lines paralleling bony landmarks)
- nodular (many small dots)
- rings or cysts
- ground glass
- consolidation (diffuse opacity with air bronchograms)
- location (where is the lesion worst?)
- upper (e.g., sarcoid, tuberculosis, silicosis/pneumoconiosis, ankylosing spondylitis, Langerhans cell histiocytosis)
- lower (e.g., cryptogenic fibrosing alveolitis, connective tissue disease, asbestosis, drug reactions)
- central (e.g., pulmonary edema, alveolar proteinosis, lymphoma, Kaposi's sarcoma, PCP)
- peripheral (e.g., cryptogenic fibrosing alveolitis, connective tissue disease, chronic eosinophilic pneumonia, bronchiolitis obliterans organizing pneumonia)
- lung volume
- increased (e.g., Langerhans cell histiocytosis, lymphangioleiomyomatosis, cystic fibrosis, allergic bronchopulmonary aspergillosis)
- decreased (e.g., fibrotic lung disease, chronic sarcoidosis, chronic extrinsic allergic alveolitis)
Pleural effusions may occur with cancer, sarcoid, connective tissue diseases and lymphangioleiomyomatosis. The presence of a pleural effusion argues against pneumocystis pneumonia.
- Reticular (linear) pattern
- (sometimes called "reticulonodular" because of the appearance of nodules at the intersection of the lines, even though there are no true nodules present)
- Nodular pattern
- Cystic
-
- cryptogenic fibrosing alveolitis (late stage "honeycomb lung")
- cystic bronchiectasis
- Langerhans cell histiocytosis
- lymphangioleiomyomatosis

- Ground glass
- Consolidation
-
- pneumonia
- alveolar haemorrhage
- alveolar cell carcinoma
- vasculitis
Signs
[edit]- The silhouette sign is especially helpful in localizing lung lesions. (e.g., loss of right heart border in right middle lobe pneumonia),[9]
- The air bronchogram sign, where branching radiolucent columns of air corresponding to bronchi is seen, usually indicates air-space (alveolar) disease, as from blood, pus, mucus, cells, protein surrounding the air bronchograms. This is seen in Respiratory distress syndrome[9]
Disease mimics
[edit]Disease mimics are visual artifacts, normal anatomic structures or harmless variants that may simulate diseases and abnormalities.
-
![A prominent thymus, which can give the impression of a widened mediastinum.[10]](//upload.wikimedia.org/wikipedia/commons/thumb/c/c7/X-ray_of_an_infant_with_a_prominent_thymus.jpg/120px-X-ray_of_an_infant_with_a_prominent_thymus.jpg)
-
 The inferior skin folds of the supraclavicular fossa may give the impression of a periosteal reaction of the clavicle
The inferior skin folds of the supraclavicular fossa may give the impression of a periosteal reaction of the clavicle
![A prominent thymus, which can give the impression of a widened mediastinum.[10]](https://en.wikipedia.org/wiki/File:X-ray_of_an_infant_with_a_prominent_thymus.jpg)

Limitations
[edit]While chest radiographs are a relatively cheap and safe method of investigating diseases of the chest, there are a number of serious chest conditions that may be associated with a normal chest radiograph and other means of assessment may be necessary to make the diagnosis. For example, a patient with an acute myocardial infarction may have a completely normal chest radiograph.
Gallery
[edit]-
 Chest X-ray PA inverted and enhanced.
Chest X-ray PA inverted and enhanced. -
 Projectionally rendered CT scan, showing the transition of thoracic structures between the anteroposterior and lateral view
Projectionally rendered CT scan, showing the transition of thoracic structures between the anteroposterior and lateral view -
 Chest film showing increased opacity in both lungs, indicative of pneumonia
Chest film showing increased opacity in both lungs, indicative of pneumonia -
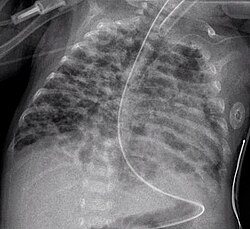 A chest radiograph showing bronchopulmonary dysplasia.
A chest radiograph showing bronchopulmonary dysplasia. -
 A chest film after insertion of an implantable cardioverter-defibrillator, showing the shock generator in the upper left chest and the electrical lead inside the right heart. Note both radio-opaque coils along the device lead.
A chest film after insertion of an implantable cardioverter-defibrillator, showing the shock generator in the upper left chest and the electrical lead inside the right heart. Note both radio-opaque coils along the device lead. -
 Portable chest (ie, antero-posterior view) showing endotracheal tube and Levin tube, both properly in place.
Portable chest (ie, antero-posterior view) showing endotracheal tube and Levin tube, both properly in place.

.gif)




References
[edit]- ^ Fred A. Mettler, Walter Huda, Terry T. Yoshizumi, Mahadevappa Mahesh: "Effective Doses in Radiology and Diagnostic Nuclear Medicine: A Catalog" – Radiology 2008;248:254–263
- ^ "Radiation Dose in X-Ray and CT Exams". radiologyinfo.org by the Radiological Society of North America. Retrieved 2017-08-10.
- ^ Using Digital Chest Images to Monitor the Health of Coal Miners and Other Workers Archived 2019-01-28 at the Wayback Machine. National Institute for Occupational Safety and Health.
- ^ medicalmnemonics.com > Chest X-ray interpretation Archived January 13, 2010, at the Wayback Machine 2002
- ^ "Chest X-ray quality – Projection". Radiology Masterclass. Retrieved 27 January 2016.
- ^ Bush, A; Gray, H; Denison, DM (February 1988). "Diagnosis of pulmonary hypertension from radiographic estimates of pulmonary arterial size". Thorax. 43 (2): 127–31. doi:10.1136/thx.43.2.127. PMC 1020754. PMID 3353884.
- ^ Gibbs, JM; Chandrasekhar, CA; Ferguson, EC; Oldham, SA (2007). "Lines and stripes: where did they go?--From conventional radiography to CT". Radiographics. 27 (1): 33–48. doi:10.1148/rg.271065073. PMID 17234997.
- ^ Gandhi, Sanjay (December 7, 2013). Chest Radiology: Exam Revision Made Easy (1st ed.). JMD Books. pp. 541 pages.
- ^ a b Chest X-Ray, OB-GYN 101: Introductory Obstetrics & Gynecology. © 2003, 2004, 2005, 2008 Medical Education Division, Brookside Associates, Ltd. Retrieved 9 February 2010.
- ^ Khan, Nausheen; Thebe, Dimakatso C.; Suleman, Farhanah; Van de Werke, Irma (2015). "Pitfalls and mimics: The many facets of normal paediatric thymus". South African Journal of Radiology. 19 (1). doi:10.4102/sajr.v19i1.803. ISSN 2078-6778. (CC BY 4.0)
External links
[edit]- Chest X-ray Atlas
- USUHS: Basic Chest X-Ray Review
- eMedicine Radiology: Chest articles
- Database of chest radiology related to emergency medicine Archived 2008-07-25 at the Wayback Machine
- Introduction to chest radiology: a tutorial for learning to read a chest x-ray
- Chest Radiology Tutorials Free Web Tutorials for Chest Anatomy and Lung Malignancies in Radiology
- Yale: Introduction to Cardiothoracic Imaging
Chest radiograph
View on GrokipediaOverview
Definition and Purpose
A chest radiograph, commonly abbreviated as CXR, is a two-dimensional projection X-ray image of the chest that captures key structures including the lungs, heart, ribs, and diaphragm.[4][5] This imaging modality serves as a foundational diagnostic tool in medical practice, providing a non-invasive means to visualize thoracic anatomy.[6] The term "radiograph" derives from the Latin "radius" meaning ray and Greek "-graphy" meaning writing or recording, reflecting the process of capturing images through radiation.[7] The procedure employs ionizing radiation, typically X-rays, which pass through the body and are differentially absorbed by tissues based on their density and atomic number, resulting in grayscale images.[8] In these images, low-density structures like air in the lungs appear black due to minimal attenuation, while high-density tissues such as bone appear white from greater absorption of the radiation beam.[9] This contrast enables differentiation of anatomical features and potential abnormalities.[10] The primary purposes of a chest radiograph include the initial assessment of respiratory symptoms like shortness of breath or persistent cough, evaluation of cardiac conditions, detection of trauma-related injuries, and monitoring of chronic illnesses affecting the thorax.[6][4] It is often the first-line imaging study due to its accessibility, low cost, and ability to provide rapid diagnostic insights in both acute and routine clinical settings.[11] Common abbreviations also encompass PA chest X-ray, referring to the standard posteroanterior projection.[12]Historical Development
The discovery of X-rays by Wilhelm Conrad Röntgen on November 8, 1895, marked the foundational event in the development of chest radiography, as he observed these rays penetrating materials to produce shadow images on fluorescent screens during experiments with cathode-ray tubes at the University of Würzburg.[13] Röntgen's subsequent publication in December 1895 detailed the properties of these "X-rays," leading to rapid medical adoption; the first radiographic image was of his wife's hand, revealing skeletal structures, and by 1896, X-rays were applied to visualize lung pathologies.[13] In the early 1900s, chest radiography emerged as a critical tool for tuberculosis (TB) screening, a leading cause of death at the time, enabling non-invasive detection of pulmonary infiltrates and cavities in sanatoria and public health initiatives across Europe and North America.[14] During World War I (1914–1918), the introduction of portable X-ray units revolutionized battlefield imaging, including chest examinations for TB and trauma-related lung injuries, with physicist Marie Curie developing over 20 mobile "Little Curies" vehicles equipped with X-ray generators and darkrooms to scan wounded soldiers near the front lines.[15] These units facilitated rapid diagnosis amid resource constraints, saving countless lives by identifying conditions like pneumothorax and early TB reactivation in troops. In the 1920s, advancements in film-screen systems improved chest image quality and accessibility; Kodak's introduction of cellulose triacetate-based film replaced flammable nitrate bases, while latitude-type films were optimized for the wide density range in chest exams, from aerated lungs to dense mediastinum, enabling mass screening programs.[16] The 1930s saw standardization of chest X-ray protocols amid intensified TB campaigns, with mass miniature radiography (using photofluorography on small films) deployed in mobile units like buses to screen millions in industrialized nations, establishing systematic PA and lateral views for consistent interpretation.[17] Radiologists such as those in the U.S. Public Health Service contributed to protocols emphasizing double-reading to reduce false positives, supporting global efforts that screened over 100 million individuals by the decade's end. The shift to digital radiography began with computed radiography (CR) in 1983, when Fuji introduced the first photostimulable phosphor system, allowing laser scanning of storage plates to produce digital images and eliminating wet chemical processing for faster chest workflows.[18] Direct digital radiography (DR) emerged in the late 1990s and proliferated in the 2000s with flat-panel detectors, enabling real-time acquisition without intermediate plates; by the mid-2000s, amorphous selenium and cesium iodide panels were standard for chest imaging, reducing processing time from minutes to seconds and improving dynamic range for better visualization of subtle lung abnormalities while lowering radiation doses by up to 50% compared to film-screen systems.[19] These innovations enhanced image quality, supported computer-aided detection, and facilitated telemedicine in TB-endemic regions.[19]Acquisition and Technique
Patient Preparation and Positioning
Patient preparation for a chest radiograph begins with informing the individual about the procedure to alleviate anxiety and ensure cooperation, as clear communication helps minimize movement artifacts during imaging. No fasting or special dietary restrictions are required prior to the examination. Patients are instructed to remove jewelry, eyeglasses, dental appliances, and any metal objects or clothing that could create artifacts on the image, and they may be asked to wear a loose-fitting gown for the procedure. Women of childbearing age should inform the technologist if there is any possibility of pregnancy to allow for appropriate precautions. Standard positioning for the posteroanterior (PA) view involves the patient standing erect with their chest pressed firmly against the image receptor, chin slightly elevated to avoid overlap with the neck, and hands placed on the hips with palms outward and shoulders rolled forward to rotate the scapulae away from the lung fields. The patient is instructed to take a deep breath and hold it at full inspiration to expand the lungs fully, enabling visualization of approximately 5 to 7 anterior ribs above the diaphragm, which reduces vascular crowding and improves diagnostic quality. For the lateral view, the patient stands with their left side against the receptor, arms raised and crossed above the head, again at full inspiration to optimize lung expansion. For patients unable to stand, such as those who are bedridden or in trauma settings, an anteroposterior (AP) supine projection is performed with the patient lying flat on their back, using a portable unit if necessary, though this may result in magnification of the heart and mediastinum. In lateral decubitus views, used to assess for free pleural fluid or air, the patient lies on their side for several minutes prior to imaging to allow redistribution, with expiration sometimes employed to enhance detection of small effusions by reducing lung volume. Special considerations apply to pediatric patients, where immobilization techniques such as swaddling or parental holding with lead apron protection may be used to prevent motion, and sedation is rarely required for routine chest radiographs due to the brevity of the procedure. For pregnant patients, the examination is justified only if essential, with efforts to adhere to the ALARA (as low as reasonably achievable) principle for radiation exposure; recent guidelines recommend against routine fetal shielding as it can obscure diagnostic areas without significant dose reduction benefit, and a single frontal view may suffice in some cases. Elderly or mobility-impaired individuals, including trauma cases, often require assistive devices or supine positioning to ensure safety and feasibility, with technologists providing support to maintain alignment.Imaging Process and Radiation Exposure
The imaging process for a chest radiograph begins with an X-ray tube, consisting of a cathode that emits electrons and an anode that serves as the target for electron acceleration, generating X-rays through bremsstrahlung and characteristic radiation.[20] These X-rays are directed toward the patient, with collimation used to restrict the beam to the chest area (typically 35 x 43 cm for a posteroanterior view), minimizing scatter radiation and unnecessary exposure to surrounding tissues.[20] The attenuated X-ray beam, after passing through the patient's thorax, is captured by a detector: traditional analog systems use film-screen combinations, while modern digital systems employ flat-panel detectors (either indirect conversion with scintillators like cesium iodide or direct conversion with materials such as amorphous selenium) or computed radiography plates with storage phosphors.[20] The central ray is aligned perpendicular to the detector to ensure accurate projection.[20] Key technical parameters govern the quality and safety of the image. Kilovoltage peak (kVp) typically ranges from 100 to 125 for chest imaging to achieve sufficient penetration through air-filled lungs while maintaining contrast; higher kVp values increase beam energy, reduce absorption in bone, and lower the required dose but decrease image contrast.[20] Milliampere-seconds (mAs), the product of tube current and exposure time, controls the quantity of X-rays produced and is usually set at 2-8 mAs for an average adult chest, adjusting for patient size to optimize density without overexposure.[21] An anti-scatter grid, often with a ratio of 10:1 to 12:1 and at least 103 lines per inch, is routinely used in adult chest radiography to absorb scattered photons and enhance contrast by reducing fogging.[20] Radiation exposure in chest radiography adheres to the ALARA (As Low As Reasonably Achievable) principle, which emphasizes minimizing dose while preserving diagnostic utility through optimized protocols, shielding, and equipment calibration.[22] The typical effective dose for a single posteroanterior chest view is approximately 0.02 mSv (range 0.01-0.04 mSv), equivalent to about 1-5 days of natural background radiation (global average ~2.4 mSv annually; ~3 mSv in the U.S.).[22][23][24] This low dose reflects the high inherent sensitivity of chest imaging to X-rays due to low tissue density, with variations depending on patient habitus and technique.[24] Digital radiography differs from analog systems primarily in detection and processing capabilities, enabling post-acquisition enhancements that improve interpretability without additional exposure. Analog film-screen radiography relies on fixed chemical processing with limited dynamic range (1:40), often requiring repeats for suboptimal exposures, whereas digital systems offer a wider latitude (1:100 to 1:1000), allowing adjustments to contrast, brightness, and edge enhancement tailored to chest structures like pulmonary vessels.[25] This post-processing reduces the need for retakes, further supporting dose reduction, and facilitates integration with picture archiving and communication systems (PACS) for efficient storage and retrieval.[25]Projections and Views
Standard Views
The standard routine chest radiograph typically consists of posteroanterior (PA) and lateral projections, providing comprehensive frontal and side views of the thorax.[12] The posteroanterior (PA) view is the primary standard projection in chest radiography, where the x-ray beam passes from the posterior to the anterior aspect of the patient, who stands upright facing the image receptor with hands on hips or hugging the receptor to rotate shoulders forward and depress scapulae away from lung fields.[26] This positioning minimizes magnification of cardiac and mediastinal structures, providing accurate assessment of heart size (typically less than half the thoracic diameter) and clear visualization of lung fields during suspended full inspiration, which allows visualization of at least 10 posterior ribs.[26][27] The anteroposterior (AP) view serves as an alternative projection when upright positioning is not feasible, such as in portable bedside imaging for critically ill patients, with the x-ray beam directed from anterior to posterior while the patient sits or stands with back against the receptor and hands at sides.[28][27] This approach, however, increases the object-to-image distance for the heart, resulting in magnification of the cardiac shadow (up to 15-20% larger than in PA views) and potential distortion of lung bases due to beam divergence and shorter source-to-image distances often used in portable setups.[28][27] The lateral view, typically acquired as a left profile with the patient standing or supine, provides a sagittal perspective that is essential for evaluating the retrosternal and retrocardiac spaces, which are superimposed on frontal projections.[29] This projection aids in assessing hilar overlap and clarifying the position of abnormalities relative to mediastinal contours, such as distinguishing anterior from posterior lesions.[30] It is particularly valuable for delineating the retrosternal clear space and retrocardiac silhouette, where deviations in lucency can indicate underlying pathology.[31] Exposure and quality criteria for standard chest views emphasize proper centering at the T4 vertebral level to ensure symmetric visualization of the thorax, with a source-to-image distance of 72 inches (183 cm) to reduce magnification and improve sharpness of pulmonary vasculature and mediastinal contours.[32][33] Collimation should limit the field to 5 cm above the shoulders, to the 12th rib inferiorly, and to the lateral skin margins, using high kVp (100-110) techniques to penetrate mediastinal structures while maintaining contrast in lung fields.[26][28] Optimal images demonstrate no rotation (symmetric clavicle distances from spinous processes), full inspiration without patient motion, and clear demarcation of diaphragmatic domes.[26][27]Supplemental Views
Supplemental views in chest radiography are additional projections employed to address specific diagnostic queries or to resolve ambiguities identified on standard posteroanterior (PA) or anteroposterior (AP) views, enhancing visualization of obscured structures without routinely supplanting primary imaging.[31] The lordotic view, a supplemental projection for apical evaluation, involves the patient leaning backward at approximately 45 degrees with the upper back, shoulders, and head against the receptor while arching the back to project the clavicles and first ribs above the lung apices.[34] This technique enhances visualization of upper lobe pathology, such as tumors or tuberculosis, that may be obscured by overlying bony structures in standard PA or AP views.[34][27] Oblique views involve rotating the patient approximately 45 degrees from the frontal plane, either anteriorly or posteriorly, to project structures away from overlap and improve diagnostic yield in targeted scenarios.[35] Anterior oblique positioning is commonly used to isolate the axillary portions of the ribs, facilitating the detection of fractures that may be obscured on standard views.[36] Posterior oblique views similarly separate superimposed thoracic elements, such as ribs or pulmonary opacities, allowing better characterization of potential injuries or abnormalities.[37] Decubitus views position the patient lying on their side—right lateral decubitus for the left side or left lateral decubitus for the right—to leverage gravity in assessing fluid dynamics within the pleural space.[38] This projection is primarily indicated to evaluate free-flowing pleural effusions, as layering fluid becomes apparent along the dependent hemithorax after a brief exposure interval, distinguishing mobile collections from adherent or loculated ones.[37] It also aids in detecting small pneumothoraces by allowing air to rise to the non-dependent side.[38] Fluoroscopic or older tomographic techniques, though rarely utilized in contemporary practice due to advancements in computed tomography, historically supplemented static radiographs for dynamic evaluations, such as assessing diaphragm motion during respiration.[39] Real-time fluoroscopy enables observation of diaphragmatic excursion, particularly in the sniff test maneuver, to identify paradoxical movement indicative of dysfunction.[40] These methods provide functional insights but are largely supplanted by ultrasound or MRI for such purposes. Additional views inherently contribute to cumulative radiation exposure, though increments are typically minimal compared to standard protocols.[31]Normal Anatomy
Key Anatomical Landmarks
In a normal chest radiograph, the bony structures provide the foundational framework for identifying thoracic anatomy. The clavicles appear as symmetric, curved horizontal bones projecting laterally from the manubrium, positioned superior to the lung apices and serving as reference points for assessing mediastinal widening. The ribs form a series of arched, paired bony structures encircling the thorax; typically, 10 posterior ribs are visible above the diaphragm on adequate inspiration, with the posterior aspects more clearly delineated due to their alignment with the spine. The thoracic spine is seen as a central, vertical column of vertebral bodies and intervertebral spaces, appearing more radiolucent inferiorly on lateral projections due to overlying lung tissue. The scapulae are superimposed over the upper lung fields as irregular, triangular bony shadows, with their medial borders often distinguishable from adjacent pleural lines. Soft tissue landmarks delineate the mediastinal and diaphragmatic contours. The heart borders are formed by the right atrium on the right side, presenting a smooth vertical interface, and the left ventricle on the left, contributing to the cardiomediastinal silhouette that occupies less than half the thoracic diameter at the level of the diaphragm. The diaphragm domes appear as smooth, upward-curving structures, with the right dome positioned slightly higher than the left due to the underlying liver, both sharply defined against the aerated lung bases. The trachea is visible as a midline radiolucent column descending from the thoracic inlet, bifurcating at the carina—typically at the level of the T4-T5 vertebrae—where it divides into the main bronchi, observable as a subtle Y-shaped junction on lateral views. The lungs are divided into zones corresponding to the lobes, facilitating zonal assessment of parenchymal patterns. The upper lobes occupy the apical regions above the horizontal fissure on the right and the oblique fissure on the left, showing finer vascular markings peripherally; the middle lobe on the right and lingula on the left lie medially between the fissures, adjacent to the heart border; the lower lobes fill the basal areas below the fissures, extending to the diaphragm with more prominent vascularity. The hila, located centrally at the lung roots, contain the pulmonary arteries and veins branching into the lung parenchyma; the left hilum is typically higher than the right, both appearing as well-defined, convex densities with smooth margins on posteroanterior views. Vascular structures outline the great vessels within the mediastinum. The aortic arch is visualized as a prominent, curvilinear left superior mediastinal contour, arching over the left main bronchus before descending. The descending aorta appears as a vertical, soft-tissue density paralleling the left side of the spine, posterior to the heart on lateral projections. The superior vena cava is seen as a right superior mediastinal vertical structure, draining into the right atrium and forming a smooth interface with the right heart border. These landmarks are primarily evaluated on standard posteroanterior and lateral projections for optimal visualization.Systematic Interpretation Approach
A systematic interpretation approach ensures consistent evaluation of chest radiographs by radiologists and clinicians, minimizing errors through structured assessment of image quality and anatomical regions. One widely adopted framework is the ABCDE method, adapted from trauma assessment protocols, which guides reviewers to evaluate key components sequentially.[41] In the ABCDE method, the process begins with A: Airway, assessing tracheal alignment (typically midline or slightly to the right) and patency from the larynx to the carina, noting any deviation or narrowing that could indicate mass effect or obstruction. Next, B: Breathing involves examining the lung fields for symmetry, opacities, and overall expansion, ensuring clear visualization of the lung zones and pleural spaces relative to anatomical landmarks such as the hila and fissures. C: Circulation focuses on the heart size (cardiothoracic ratio ideally less than 0.5 on posteroanterior views) and vascular markings, checking for mediastinal widening or pulmonary vascular congestion. D: Disability evaluates bones and soft tissues, including ribs, clavicles, spine, and surrounding structures for fractures, densities, or asymmetries. Finally, E: Exposure confirms full visualization of the lung fields, including apices and costophrenic angles, to avoid truncation of findings.[42][43] Prior to detailed analysis, image quality must be assessed using checklists to determine adequacy. Adequate inspiration is indicated by visualization of at least 6 anterior ribs or 9-10 posterior ribs above the diaphragm, preventing underinflation that could simulate pathology. Rotation is evaluated by ensuring spinous processes align midway between the medial ends of the clavicles, as misalignment can distort mediastinal contours. Penetration is sufficient if vascular markings are visible to the peripheral lung zones and vertebral disc spaces are faintly discernible through the cardiac silhouette, avoiding over- or under-exposure that obscures subtle details.[43][44][41] Common pitfalls include overlooking subtle asymmetries in lung density or vascularity due to perceptual errors, which can be mitigated by adhering to the systematic method. Comparison with prior images is essential, as it enhances detection of interval changes, such as evolving opacities or device migrations, reducing diagnostic misses in serial evaluations.[45][46][47] Picture Archiving and Communication Systems (PACS) and digital tools play a crucial role in modern interpretation by enabling magnification of regions of interest, windowing adjustments for contrast optimization, and side-by-side comparison with priors, thereby improving accuracy and efficiency in detecting fine details without additional radiation exposure.[48][43]Pathological Findings
Nodules and Masses
In chest radiography, a pulmonary nodule is defined as a well-circumscribed, rounded opacity measuring up to 3 cm in diameter, surrounded by aerated lung, while a mass exceeds 3 cm and may obscure adjacent structures.[49] These opacities appear as discrete densities within the lung fields, often detected incidentally during routine imaging. Nodules and masses can be solitary or multiple, with characteristics such as margin definition, internal features, and location providing clues to their etiology; for instance, spiculated or irregular margins suggest malignancy, whereas smooth, well-defined borders are more typical of benign lesions.[50] Calcification patterns within the nodule—such as central, laminated, or popcorn types—favor benignity, often indicating prior granulomatous infection or hamartoma, while cavitation (a gas-filled cavity within the lesion) may occur in both benign (e.g., abscess) and malignant processes but requires further evaluation.[51] Pulmonary nodules are an uncommon incidental finding on chest radiographs, with reported frequencies of approximately 0.1-0.2% in general populations undergoing imaging for various reasons.[52] In higher-risk screening contexts using CT, such as those evaluating for lung cancer or infection, the detection rate can approach 10% or more, underscoring their prevalence as a diagnostic challenge. The differential diagnosis distinguishes benign from malignant causes: benign nodules include hamartomas (often with fat or popcorn calcification) and granulomas (from infections like tuberculosis or histoplasmosis, frequently calcified), while malignant ones encompass primary lung carcinomas (e.g., adenocarcinoma or squamous cell) and metastases from extrathoracic primaries like breast or colon cancer.[50] Growth rate assessment via serial chest radiographs is crucial for characterization, particularly for larger nodules (>1.5-2 cm), where a volume doubling time of 30-400 days suggests malignancy, though smaller lesions often require computed tomography (CT) for precise measurement due to radiographic limitations.[53] Management of nodules detected on chest radiographs follows size-based guidelines adapted from expert consensus, such as those from the Fleischner Society, which primarily address incidental CT findings but inform radiographic follow-up. For low-risk patients with nodules <6 mm, no routine follow-up is typically recommended unless high-risk features are present; nodules 6-8 mm warrant optional CT at 6-12 months, while those >8 mm or with suspicious morphology (e.g., spiculation) prompt immediate CT evaluation or biopsy. The American College of Chest Physicians (ACCP) guidelines emphasize reviewing prior radiographs for stability before advancing to CT, as stable nodules over two years are likely benign with >95% certainty.[53] Supplemental views, such as lateral projections, may aid in localizing nodules relative to fissures or hila to refine the differential. Overall, while chest radiography excels at initial detection, confirmatory imaging with CT is essential for most cases to guide risk stratification and intervention.Cavitary Lesions
Cavitary lesions on chest radiographs appear as lucent, gas-filled spaces surrounded by a wall, typically within areas of pulmonary consolidation or mass, distinguishing them from solid nodules or cysts by their hollow nature. The wall thickness is a key radiographic feature: thin-walled cavities (≤4 mm) are often benign, seen in conditions like bullae or chronic infections such as tuberculosis, while thick-walled cavities (>4 mm, particularly >15 mm) more commonly indicate infection or malignancy, with studies showing 94% of thin-walled lesions as nonmalignant and 90% of thick-walled ones as malignant.[54][55] Common etiologies include infectious processes, such as necrotizing pneumonia from bacteria like Staphylococcus aureus or Klebsiella pneumoniae, fungal infections including aspergilloma (a mycetoma within a preexisting cavity), and tuberculosis, which causes cavitation in 30-50% of cases. Malignant causes, particularly squamous cell carcinoma of the lung (with cavitation in 7-11% of primary tumors) and metastatic lesions (4% cavitation rate), often present with irregular, thick walls. Vascular etiologies, such as pulmonary infarction from embolism, account for 2.7-7% of cavities and typically show peripheral location.[54][56][55] Associated radiographic signs include air-fluid levels, visible in upright views within cavities due to layering of fluid or pus, as seen in abscesses or aspergillomas, and surrounding parenchymal consolidation or opacification, which is frequent in infectious causes like necrotizing pneumonia or tuberculosis. Diagnostic clues on chest radiographs involve lesion location—upper lobe predominance suggesting tuberculosis or post-primary infections—and multiplicity, where multiple cavities may indicate septic emboli, disseminated fungal disease, or metastases. Standard posteroanterior and lateral views are essential for projecting cavities and assessing these features.[54][56]Pleural Abnormalities
Pleural abnormalities on chest radiographs encompass deviations in the pleural space, such as accumulations of fluid, air, or fibrotic changes, which can alter the normal appearance of the lung margins and costophrenic angles.[57] These findings are crucial for identifying conditions like effusions, pneumothoraces, and thickenings, often requiring correlation with clinical history for accurate diagnosis.[58] Pleural EffusionA pleural effusion appears as an opacity in the dependent portions of the thorax on upright posteroanterior chest radiographs, with blunting of the costophrenic angles being an early sign detectable with as little as 175-200 mL of fluid.[59] The classic meniscus sign, characterized by a curved upper border of the fluid higher laterally than medially, indicates a more substantial effusion exceeding 200 mL and helps distinguish it from other opacities.[59] On lateral decubitus views, layering of the fluid confirms the presence of free-flowing effusion, allowing detection of smaller volumes as low as 50 mL, which may not be apparent on standard views.[59] Effusions are quantified as small (less than 200 mL, often subpulmonic or minimal blunting) or large (greater than 500 mL, causing significant hemithorax opacification), though ultrasound provides superior accuracy for volume estimation compared to radiography, with correlation coefficients of r=0.80 for sonography versus r=0.47 for chest x-ray.[60] Pneumothorax
Pneumothorax is identified by the presence of a thin, sharp visceral pleural line parallel to the chest wall, separated by a lucent area devoid of lung markings, indicating air in the pleural space.[61] This line is most conspicuous apically on upright inspiratory radiographs, with the absence of vascular markings beyond it confirming the diagnosis; small pneumothoraces may measure 2-3 cm at the apex.[62] In tension pneumothorax, a life-threatening variant, the pneumothorax causes complete lung collapse and mediastinal shift toward the contralateral side, often with deep sulcus sign at the costophrenic angle on supine views.[61] Supplemental expiratory views can enhance visibility of small pneumothoraces by reducing lung volume.[63] Pleural Thickening
Pleural thickening manifests as irregular or linear opacities along the chest wall or diaphragm, resulting from fibrosis due to prior inflammation, infection, or hemorrhage.[64] In asbestos exposure, characteristic bilateral pleural plaques appear as discrete, calcified or non-calcified areas of parietal pleural thickening, typically dome-shaped and localized to the posterolateral chest wall or diaphragmatic surfaces, without involving the mediastinum.[64] Diffuse pleural thickening, often encasing more than a quarter of the chest wall, blunts costophrenic angles and may stem from resolved effusions or chronic inflammation, distinguishing it from focal plaques.[65] These changes are usually asymptomatic but serve as markers of prior exposure or injury.[64]