Recent from talks
Ciliary muscle
Knowledge base stats:
Talk channels stats:
Members stats:
Ciliary muscle
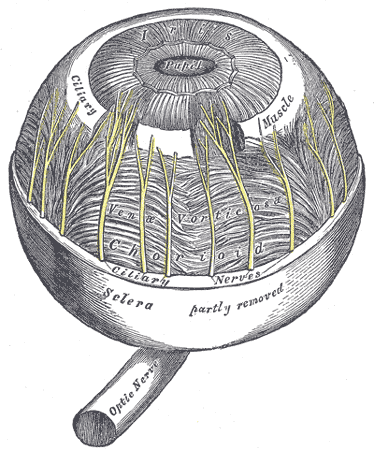
The ciliary muscle is an intrinsic muscle of the eye formed as a ring of smooth muscle in the eye's middle layer, the uvea (vascular layer). It controls accommodation for viewing objects at varying distances and regulates the flow of aqueous humor into Schlemm's canal. It also changes the shape of the lens within the eye but not the size of the pupil which is carried out by the sphincter pupillae muscle and dilator pupillae.
The ciliary muscle, pupillary sphincter muscle and pupillary dilator muscle sometimes are called intrinsic ocular muscles or intraocular muscles.
The ciliary muscle develops from mesenchyme within the choroid and is considered a cranial neural crest derivative.
The ciliary muscle receives parasympathetic fibers from the short ciliary nerves that arise from the ciliary ganglion. The parasympathetic postganglionic fibers are part of cranial nerve V1 (Nasociliary nerve of the trigeminal), while presynaptic parasympathetic fibers to the ciliary ganglia travel with the oculomotor nerve. The postganglionic parasympathetic innervation arises from the ciliary ganglion.
Presynaptic parasympathetic signals that originate in the Edinger-Westphal nucleus are carried by cranial nerve III (the oculomotor nerve) and travel through the ciliary ganglion via the postganglionic parasympathetic fibers which travel in the short ciliary nerves and supply the ciliary body and iris. Parasympathetic activation of the M3 muscarinic receptors causes ciliary muscle contraction. The effect of contraction is to decrease the diameter of the ring of ciliary muscle causing relaxation of the zonule fibers, the lens becomes more spherical, increasing its power to refract light for near vision.[citation needed]
The parasympathetic tone is dominant when a higher degree of accommodation of the lens is required, such as reading a book.
The ciliary fibers have circular (Ivanoff), longitudinal (meridional) and radial orientations.
According to Hermann von Helmholtz's theory, the circular ciliary muscle fibers affect zonular fibers in the eye (fibers that suspend the lens in position during accommodation), enabling changes in lens shape for light focusing. When the ciliary muscle contracts, it pulls itself forward and moves the frontal region toward the axis of the eye. This releases the tension on the lens caused by the zonular fibers (fibers that hold or flatten the lens). This release of tension of the zonular fibers causes the lens to become more spherical, adapting to short range focus. Conversely, relaxation of the ciliary muscle causes the zonular fibers to become taut, flattening the lens, increasing the focal distance, increasing long range focus. Although Helmholtz's theory has been widely accepted since 1855, its mechanism still remains controversial. Alternative theories of accommodation have been proposed by others, including L. Johnson, M. Tscherning, and especially Ronald A. Schachar.
Hub AI
Ciliary muscle AI simulator
(@Ciliary muscle_simulator)
Ciliary muscle
The ciliary muscle is an intrinsic muscle of the eye formed as a ring of smooth muscle in the eye's middle layer, the uvea (vascular layer). It controls accommodation for viewing objects at varying distances and regulates the flow of aqueous humor into Schlemm's canal. It also changes the shape of the lens within the eye but not the size of the pupil which is carried out by the sphincter pupillae muscle and dilator pupillae.
The ciliary muscle, pupillary sphincter muscle and pupillary dilator muscle sometimes are called intrinsic ocular muscles or intraocular muscles.
The ciliary muscle develops from mesenchyme within the choroid and is considered a cranial neural crest derivative.
The ciliary muscle receives parasympathetic fibers from the short ciliary nerves that arise from the ciliary ganglion. The parasympathetic postganglionic fibers are part of cranial nerve V1 (Nasociliary nerve of the trigeminal), while presynaptic parasympathetic fibers to the ciliary ganglia travel with the oculomotor nerve. The postganglionic parasympathetic innervation arises from the ciliary ganglion.
Presynaptic parasympathetic signals that originate in the Edinger-Westphal nucleus are carried by cranial nerve III (the oculomotor nerve) and travel through the ciliary ganglion via the postganglionic parasympathetic fibers which travel in the short ciliary nerves and supply the ciliary body and iris. Parasympathetic activation of the M3 muscarinic receptors causes ciliary muscle contraction. The effect of contraction is to decrease the diameter of the ring of ciliary muscle causing relaxation of the zonule fibers, the lens becomes more spherical, increasing its power to refract light for near vision.[citation needed]
The parasympathetic tone is dominant when a higher degree of accommodation of the lens is required, such as reading a book.
The ciliary fibers have circular (Ivanoff), longitudinal (meridional) and radial orientations.
According to Hermann von Helmholtz's theory, the circular ciliary muscle fibers affect zonular fibers in the eye (fibers that suspend the lens in position during accommodation), enabling changes in lens shape for light focusing. When the ciliary muscle contracts, it pulls itself forward and moves the frontal region toward the axis of the eye. This releases the tension on the lens caused by the zonular fibers (fibers that hold or flatten the lens). This release of tension of the zonular fibers causes the lens to become more spherical, adapting to short range focus. Conversely, relaxation of the ciliary muscle causes the zonular fibers to become taut, flattening the lens, increasing the focal distance, increasing long range focus. Although Helmholtz's theory has been widely accepted since 1855, its mechanism still remains controversial. Alternative theories of accommodation have been proposed by others, including L. Johnson, M. Tscherning, and especially Ronald A. Schachar.
Recent media