Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
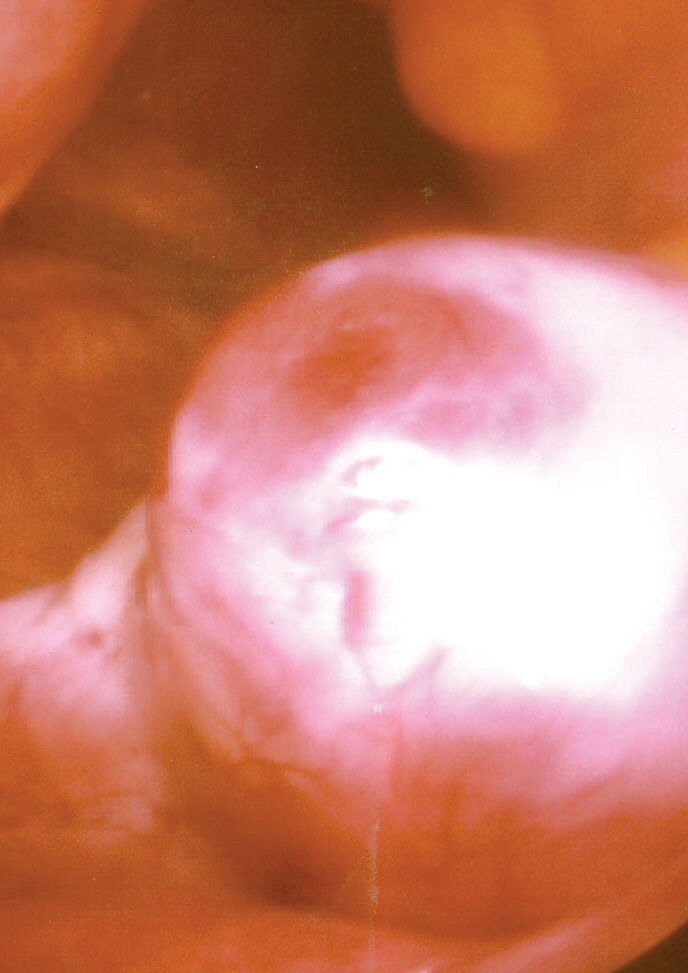
Ovulation
Ovulation is an important part of the menstrual cycle in female vertebrates where the egg cells are released from the ovaries as part of the ovarian cycle. In female humans ovulation typically occurs near the midpoint in the menstrual cycle and after the follicular phase. Ovulation is stimulated by an increase in luteinizing hormone (LH). The ovarian follicles rupture and release the secondary oocyte ovarian cells.
After ovulation, during the luteal phase, the egg will be available to be fertilized by sperm. If it is not, it will break down in less than a day. Meanwhile, the uterine lining (endometrium) continues to thicken to be able to receive a fertilized egg. If no conception occurs, the uterine lining will eventually break down and be shed from the body via the vagina during menstruation.
Some people choose to track ovulation in order to improve or aid becoming pregnant by timing intercourse with their ovulation. The signs of ovulation may include cervical mucus changes, mild cramping in the abdominal area, and a small rise in basal body temperature. Medication is also sometimes required by those experiencing infertility to induce ovulation.
Ovulation occurs about midway through the menstrual cycle, after the follicular phase. The days in which a woman is most fertile can be calculated based on the date of the last menstrual period and the length of a typical menstrual cycle. The few days surrounding ovulation (from approximately days 10 to 18 of a 28-day cycle), constitute the most fertile phase. The time from the beginning of the last menstrual period (LMP) until ovulation is, on average, 14.6 days, but with substantial variation among females and between cycles in any single female, with an overall 95% prediction interval of 8.2 to 20.5 days.
The process of ovulation is controlled by the hypothalamus of the brain and through the release of hormones secreted in the anterior lobe of the pituitary gland, luteinizing hormone (LH) and follicle-stimulating hormone (FSH). In the preovulatory phase of the menstrual cycle, the ovarian follicle will undergo a series of transformations called cumulus expansion, which is stimulated by FSH. After this is done, a hole called the stigma will form in the follicle, and the secondary oocyte will leave the follicle through this hole. Ovulation is triggered by a spike in the amount of FSH and LH released from the pituitary gland. During the luteal (post-ovulatory) phase, the secondary oocyte will travel through the fallopian tubes toward the uterus. If fertilized by a sperm, the fertilized secondary oocyte or ovum may implant there 6–12 days later.
The follicular phase (or proliferative phase) is the phase of the menstrual cycle during which the ovarian follicles mature. The follicular phase lasts from the beginning of menstruation to the start of ovulation.
For ovulation to be successful, the ovum must be supported by the corona radiata and cumulus oophorous granulosa cells. The latter undergo a period of proliferation and mucification known as cumulus expansion. Mucification is the secretion of a hyaluronic acid-rich cocktail that disperses and gathers the cumulus cell network in a sticky matrix around the ovum. This network stays with the ovum after ovulation and has been shown to be necessary for fertilization.
Estrogen levels peak towards the end of the follicular phase, around 12 and 24 hours. This, by positive feedback, causes a surge in levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). This lasts from 24 to 36 hours, and results in the rupture of the ovarian follicles, causing the oocyte to be released from the ovary.
Hub AI
Ovulation AI simulator
(@Ovulation_simulator)
Ovulation
Ovulation is an important part of the menstrual cycle in female vertebrates where the egg cells are released from the ovaries as part of the ovarian cycle. In female humans ovulation typically occurs near the midpoint in the menstrual cycle and after the follicular phase. Ovulation is stimulated by an increase in luteinizing hormone (LH). The ovarian follicles rupture and release the secondary oocyte ovarian cells.
After ovulation, during the luteal phase, the egg will be available to be fertilized by sperm. If it is not, it will break down in less than a day. Meanwhile, the uterine lining (endometrium) continues to thicken to be able to receive a fertilized egg. If no conception occurs, the uterine lining will eventually break down and be shed from the body via the vagina during menstruation.
Some people choose to track ovulation in order to improve or aid becoming pregnant by timing intercourse with their ovulation. The signs of ovulation may include cervical mucus changes, mild cramping in the abdominal area, and a small rise in basal body temperature. Medication is also sometimes required by those experiencing infertility to induce ovulation.
Ovulation occurs about midway through the menstrual cycle, after the follicular phase. The days in which a woman is most fertile can be calculated based on the date of the last menstrual period and the length of a typical menstrual cycle. The few days surrounding ovulation (from approximately days 10 to 18 of a 28-day cycle), constitute the most fertile phase. The time from the beginning of the last menstrual period (LMP) until ovulation is, on average, 14.6 days, but with substantial variation among females and between cycles in any single female, with an overall 95% prediction interval of 8.2 to 20.5 days.
The process of ovulation is controlled by the hypothalamus of the brain and through the release of hormones secreted in the anterior lobe of the pituitary gland, luteinizing hormone (LH) and follicle-stimulating hormone (FSH). In the preovulatory phase of the menstrual cycle, the ovarian follicle will undergo a series of transformations called cumulus expansion, which is stimulated by FSH. After this is done, a hole called the stigma will form in the follicle, and the secondary oocyte will leave the follicle through this hole. Ovulation is triggered by a spike in the amount of FSH and LH released from the pituitary gland. During the luteal (post-ovulatory) phase, the secondary oocyte will travel through the fallopian tubes toward the uterus. If fertilized by a sperm, the fertilized secondary oocyte or ovum may implant there 6–12 days later.
The follicular phase (or proliferative phase) is the phase of the menstrual cycle during which the ovarian follicles mature. The follicular phase lasts from the beginning of menstruation to the start of ovulation.
For ovulation to be successful, the ovum must be supported by the corona radiata and cumulus oophorous granulosa cells. The latter undergo a period of proliferation and mucification known as cumulus expansion. Mucification is the secretion of a hyaluronic acid-rich cocktail that disperses and gathers the cumulus cell network in a sticky matrix around the ovum. This network stays with the ovum after ovulation and has been shown to be necessary for fertilization.
Estrogen levels peak towards the end of the follicular phase, around 12 and 24 hours. This, by positive feedback, causes a surge in levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). This lasts from 24 to 36 hours, and results in the rupture of the ovarian follicles, causing the oocyte to be released from the ovary.