Community hub
Esophagitis
View on Wikipedia| Esophagitis | |
|---|---|
| Other names | Oesophagitis |
 | |
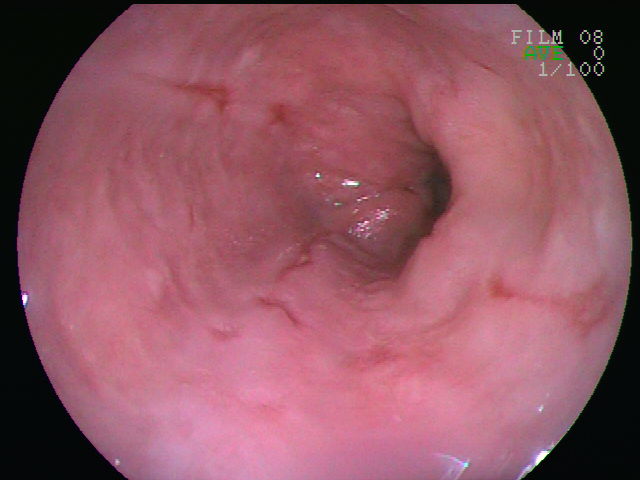
| An esophageal ulcer visualized by esophagoscopy: the reddened area at 10 o'clock on the surface of the mucosa. | |
| Specialty | Gastroenterology |
| Complications | Cancer |
Esophagitis, also spelled oesophagitis, is a disease characterized by inflammation of the esophagus. The esophagus is a tube composed of a mucosal lining, and longitudinal and circular smooth muscle fibers. It connects the pharynx to the stomach; swallowed food and liquids normally pass through it.[1]
Esophagitis can be asymptomatic; or can cause epigastric and/or substernal burning pain, especially when lying down or straining; and can make swallowing difficult (dysphagia). The most common cause of esophagitis is the reverse flow of acid from the stomach into the lower esophagus: gastroesophageal reflux disease (GERD).[2]
Signs and symptoms
[edit]The symptoms of esophagitis include:[2]
- Heartburn – a burning sensation in the lower mid-chest
- Nausea
- Dysphagia – swallowing is painful, with difficulty passing or inability to pass food through the esophagus
- Vomiting (emesis)
- Abdominal pain
- Cough
Complications
[edit]If the disease remains untreated, it can cause scarring and discomfort in the esophagus. If the irritation is not allowed to heal, esophagitis can result in esophageal ulcers. Esophagitis can develop into Barrett's esophagus and can increase the risk of esophageal cancer.[3]
Causes
[edit]Infectious esophagitis cannot be spread. However, infections can be spread by those who have infectious esophagitis. Esophagitis can develop due to many causes. GERD is the most common cause of esophagitis because of the backflow of acid from the stomach, which can irritate the lining of the esophagus.
Other causes include:
- Medicines – Can cause esophageal damage that can lead to esophageal ulcers
- Nonsteroidal anti-inflammatory drugs (NSAIDS) – aspirin, naproxen sodium, and ibuprofen. Known to irritate the GI tract.
- Antibiotics – doxycycline and tetracycline
- Quinidine
- Bisphosphonates – used to treat osteoporosis
- Steroids
- Potassium chloride
- Vitamins and supplements (iron, vitamin C, and potassium) – Supplements and minerals can be hard on the GI tract.
- Chemical injury by alkaline or acidic solutions
- Physical injury resulting from nasogastric tubes.
- Alcohol use disorder – Can wear down the lining of the esophagus.
- Crohn's disease – a type of IBD that can cause esophagitis if it attacks the esophagus.
- Stress – Can cause higher levels of acid reflux
- Radiation therapy – Can affect the immune system.
- Allergies (food, inhalants) – Allergies can stimulate eosinophilic esophagitis.
- Infection – People with immunodeficiencies have a higher chance of developing esophagitis.
- Vomiting – Acid can irritate esophagus.
- Hernias – A hernia can poke through the diaphragm muscle and can inhibit stomach acid and food from draining quickly.
- Surgery
- Eosinophilic esophagitis, a more chronic condition with a theorized autoimmune component
Mechanism
[edit]The esophagus is a muscular tube made of both voluntary and involuntary muscles. It is responsible for peristalsis of food. It is about 8 inches long and passes through the diaphragm before entering the stomach. The esophagus is made up of three layers: from the inside out, they are the mucosa, submucosa, muscularis externa. The mucosa, the inner most layer and lining of the esophagus, is composed of stratified squamous epithelium, lamina propria, and muscularis mucosae. At the end of the esophagus is the lower esophageal sphincter, which normally prevents stomach acid from entering the esophagus.
If the sphincter is not sufficiently tight, it may allow acid to enter the esophagus, causing inflammation of one or more layers. Esophagitis may also occur if an infection is present, which may be due to bacteria, viruses, or fungi; or by diseases that affect the immune system.[4]
Irritation can be caused by GERD, vomiting, surgery, medications, hernias, and radiation injury.[4] Inflammation can cause the esophagus to narrow, which makes swallowing food difficult and may result in food bolus impaction.
Diagnosis
[edit]Esophagitis can be diagnosed by upper endoscopy, biopsy, upper GI series (or barium swallow), and laboratory tests.[4]
An upper endoscopy is a procedure to look at the esophagus by using an endoscope. While looking at the esophagus, the doctor is able to take a small biopsy. The biopsy can be used to confirm inflammation of the esophagus.
An upper GI series uses a barium contrast, fluoroscopy, and an X-ray. During a barium X-ray, a solution with barium or pill is taken before getting an X-ray. The barium makes the organs more visible and can detect if there is any narrowing, inflammation, or other abnormalities that can be causing the disease. The upper GI series can be used to find the cause of GI symptoms. An esophagram is if only the throat and esophagus are looked at.[5]
Laboratory tests can be done on biopsies removed from the esophagus and can help determine the cause of the esophagitis. Laboratory tests can help diagnose a fungal, viral, or bacterial infection. Scanning for white blood cells can help diagnose eosinophil esophagitis.
Some lifestyle indicators for this disease include stress, unhealthy eating, smoking, drinking, family history, allergies, and immunodeficiency.
Types
[edit]Reflux esophagitis
Gastroesophageal reflux disease is usually assumed to be caused by inflammation from gastric acid reflux which irritates the mucosa. One study suggests that the pathogenesis of may be cytokine-mediated.[6]

Infectious esophagitis
Esophagitis happens due to a viral, fungal, parasitic or bacterial infection. More likely to happen to people who have an immunodeficiency. Types include:
Fungal
Viral
Drug-induced esophagitis
Damage to the esophagus due to medications. If the esophagus is not coated or if the medicine is not taken with enough liquid, it can damage the tissues.

Eosinophilic esophagitis
Eosinophilic esophagitis is caused by a high concentration of eosinophils in the esophagus. The presence of eosinophils in the esophagus may be due to an allergen and is often correlated with GERD. The direction of cause and effect between inflammation and acid reflux is poorly established, with recent studies (in 2016) hinting that reflux does not cause inflammation.[6] This esophagitis can be triggered by allergies to food or to inhaled allergens. This type is still poorly understood.
Lymphocytic esophagitis
Lymphocytic esophagitis is a rare and poorly understood entity associated with an increased amount of lymphocytes in the lining of the esophagus.[1] It was first described in 2006. Disease associations may include Crohn's disease, gastroesophageal reflux disease and coeliac disease. It causes similar changes on endoscopy as eosinophilic esophagitis including esophageal rings, narrow-lumen esophagus, and linear furrows.
Caustic esophagitis
Caustic esophagitis is the damage of tissue via chemical origin. This occasionally occurs through occupational exposure (via breathing of fumes that mix into the saliva which is then swallowed) or through pica.
By severity
[edit]The severity of reflux esophagitis is commonly classified into four grades according to the Los Angeles Classification:[7][8]
| Grade A | One or more mucosal breaks < 5 mm in maximal length |
| Grade B | One or more mucosal breaks > 5mm, but without continuity across mucosal folds |
| Grade C | Mucosal breaks continuous between ≥ 2 mucosal folds but involving less than 75% of the esophageal circumference |
| Grade D | Mucosal breaks involving more than 75% of esophageal circumference |
Prevention
[edit]Since there can be many causes underlying esophagitis, it is important to try to find the cause to help to prevent esophagitis. To prevent reflux esophagitis, avoid acidic foods, caffeine, eating before going to bed, alcohol, fatty meals, and smoking. To prevent drug-induced esophagitis, drink plenty of liquids when taking medicines, take an alternative drug, and do not take medicines while lying down, before sleeping, or too many at one time. Esophagitis is more prevalent in adults and does not discriminate.
Treatment
[edit]Lifestyle changes
[edit]Losing weight, stop smoking and alcohol, lowering stress, avoid sleeping/lying down after eating, raising the head of the bed, taking medicines correctly, avoiding certain medications, and avoiding foods that cause the reflux that might be causing the esophagitis.[9]
Medications
[edit]Antacids
[edit]To treat reflux esophagitis, over the counter antacids, medications that reduce acid production (H-2 receptor blockers), and proton pump inhibitors are recommended to help block acid production and to let the esophagus heal. Some prescription medications to treat reflux esophagitis include higher dose H-2 receptor blockers, proton pump inhibitors, and prokinetics, which help with the emptying of the stomach. However prokinetics are no longer licensed for GERD because their evidence of efficacy is poor, and following a safety review, licensed use of domperidone and metoclopramide is now restricted to short-term use in nausea and vomiting only.[10]
For subtypes
[edit]To treat eosinophilic esophagitis, avoiding any allergens that may be stimulating the eosinophils is recommended. As for medications, proton pump inhibitors and steroids can be prescribed. Steroids that are used to treat asthma can be swallowed to treat eosinophil esophagitis due to nonfood allergens. The removal of food allergens from the diet is included to help treat eosinophilic esophagitis.
For infectious esophagitis, medicine is prescribed based on what type of infection is causing the esophagitis. These medicines are prescribed to treat bacterial, fungal, viral, and/or parasitic infections.
Procedures
[edit]- An endoscopy can be used to remove ill fragments.
- Surgery can be done to remove the damaged part of the esophagus.[4]
- For reflux esophagitis, a fundoplication can be done to help strengthen the lower esophageal sphincter from allowing backflow of the stomach into the esophagus.
- For esophageal stricture, a gastroenterologist can perform a dilation of the esophagus.
As of 2020 evidence for magnetic sphincter augmentation is poor.[11]
Prognosis
[edit]The prognosis for a person with esophagitis depends on the underlying causes and conditions. If a patient has a more serious underlying cause such as a digestive system or immune system issue, it may be more difficult to treat. Normally, the prognosis would be good with no serious illnesses. If there are more causes than one, the prognosis could move to fair.
Terminology
[edit]The term is from Greek οἰσοφάγος "gullet" and -itis "inflammation".
References
[edit]- ^ a b "Esophagitis – Symptoms and causes – Mayo Clinic". www.mayoclinic.org. Retrieved 2017-12-13.
- ^ a b "Esophagitis-Topic Overview". WebMD. Retrieved 2017-12-13.
- ^ "Esophagitis". Johns Hopkins Medicine. 19 November 2019. Retrieved 22 July 2021.
- ^ a b c d "Understanding Esophagitis". WebMD. Retrieved 2017-11-07.
- ^ "Upper Gastrointestinal (UGI) Series". WebMD. Retrieved 2017-12-13.
- ^ a b "Inflammation, Not Acid, Cause of GERD, Study Suggests".
- ^ Farivar M. "Los Angeles Classification of Esophagitis". webgerd.com. Archived from the original on 2015-01-30. Retrieved 2010-10-27. In turn citing: Lundell LR, Dent J, Bennett JR, et al. (August 1999). "Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification". Gut. 45 (2): 172–80. doi:10.1136/gut.45.2.172. PMC 1727604. PMID 10403727.
- ^ Laparoscopic bariatric surgery, Volume 1. William B. Inabnet, Eric J. DeMaria, Sayeed Ikramuddin. ISBN 0-7817-4874-7.[page needed]
- ^ "Esophagitis". The Lecturio Medical Concept Library. Retrieved 22 July 2021.
- ^ Medicines and Healthcare Products Regulatory Agency (MHRA), 2013. Metoclopramide: risk of neurological adverse effects. Drug Safety Update 7 (1), S2. Medicines and Healthcare Products Regulatory Agency, 2014. Domperidone: risks of cardiac side effects. Drug Safety Update 7 (10), A1. Moayyedi, P., Santana, J., Khan, M., et al., 2011. Medical treatments in the short-term management of relux oesophagitis. Cochrane DB Syst. Rev. 2011 (2), Art. No. CD003244.
- ^ Kirkham, EN; Main, BG; Jones, KJB; Blazeby, JM; Blencowe, NS (January 2020). "Systematic review of the introduction and evaluation of magnetic augmentation of the lower oesophageal sphincter for gastro-oesophageal reflux disease". The British Journal of Surgery. 107 (1): 44–55. doi:10.1002/bjs.11391. PMC 6972716. PMID 31800095.
External links
[edit]| Authority control databases: National |
|---|
Esophagitis
View on GrokipediaSigns and symptoms
Typical presentations
The most common symptoms of esophagitis include dysphagia, or difficulty swallowing, which may manifest as a sensation of food sticking in the throat or chest.[1] Odynophagia, or painful swallowing, often accompanies this and can range from mild discomfort to severe pain during meals.[3] Patients frequently report heartburn, characterized by a burning sensation in the chest or throat, along with chest pain that may mimic cardiac issues.[2] Other typical presentations involve regurgitation of food or liquids, nausea, and unintended weight loss due to reduced oral intake.[5][6] Symptom presentation varies by age group, with children often exhibiting more subtle or nonspecific signs compared to adults. In infants and young children, esophagitis may present as feeding refusal, poor weight gain, or irritability during meals rather than overt swallowing difficulties.[1] Older children might show vomiting or abdominal pain, while adults more commonly experience pronounced dysphagia and food impaction.[1] Acute esophagitis typically features a sudden onset of intense symptoms, such as severe odynophagia characterized by sharp, burning, or knife-like pain behind the sternum when swallowing food, liquids, or saliva; dysphagia with a feeling of food stuck in the throat or chest, potentially leading to impaction; retrosternal pain or burning sensation that may be stabbing or dull, worsening after eating and possibly radiating to the back; heartburn and acid reflux with a sour or bitter taste in the throat or mouth; and other symptoms including sore throat, foreign body sensation, nausea, vomiting, hoarseness, or cough. Severe acute cases, such as those from corrosive or infectious causes, may also include fever, hematemesis, or melena. These symptoms, along with chest pain, can significantly impair daily functioning from the outset.[7][2] In contrast, chronic forms often involve persistent, milder symptoms like recurrent heartburn and gradual dysphagia that develop over time.[3] These symptoms can profoundly affect quality of life, including nocturnal heartburn that disrupts sleep and leads to daytime fatigue.[8] Persistent discomfort may also contribute to anxiety around eating and overall reduced well-being.[9] Untreated esophagitis may progress to complications such as esophageal strictures.[1]Complications
One of the primary complications of untreated or severe esophagitis is the development of esophageal strictures, which are areas of scarring and narrowing in the esophagus due to chronic inflammation, often leading to persistent dysphagia that impairs the passage of food and liquids.[1] These strictures, commonly resulting from prolonged gastroesophageal reflux disease (GERD)-related esophagitis, typically occur in the distal esophagus and may require endoscopic dilation procedures to restore luminal patency, with initial success rates around 80% but recurrence in 30-50% of cases despite acid suppression therapy.[10] Chronic reflux esophagitis can also progress to Barrett's esophagus, a premalignant condition characterized by the metaplastic replacement of normal squamous epithelium with intestinal-type columnar epithelium in the distal esophagus, affecting 5-12% of individuals with longstanding GERD symptoms.[11] This change increases the risk of esophageal adenocarcinoma, with annual progression rates of 0.1-0.5% in nondysplastic cases, underscoring the need for surveillance in affected patients.[11] Severe esophagitis may lead to ulceration of the esophageal mucosa, with open sores that can cause bleeding or, in rare instances, perforation, particularly in cases involving caustic ingestion or severe infectious esophagitis such as that caused by Candida or herpes simplex virus.[2] Esophageal perforation, a life-threatening event, occurs when the weakened wall tears, allowing contents to leak into surrounding tissues, and is more likely in inflamed esophagi lacking a protective serosal layer.[12] Chronic bleeding from esophageal ulcers or erosions in esophagitis can result in iron-deficiency anemia, as repeated blood loss depletes iron stores and reduces hemoglobin levels, contributing to fatigue and other systemic effects.[13] Additionally, the dysphagia and odynophagia associated with esophagitis may lead patients to avoid eating, fostering malnutrition and weight loss, while impaired swallowing increases the risk of aspiration pneumonia through inadvertent inhalation of food or gastric contents into the lungs.[14] In cases of perforation, rare but severe systemic complications such as mediastinitis can arise, involving bacterial infection and inflammation of the mediastinum from leaked esophageal contents, with an incidence of about 1% among perforations and potential for rapid progression to sepsis if not addressed promptly.[15]Epidemiology
Incidence and prevalence
Esophagitis encompasses several subtypes, with reflux esophagitis being the most common form globally, affecting approximately 20-30% of adults diagnosed with gastroesophageal reflux disease (GERD).[16] Erosive esophagitis, a key manifestation of GERD, shows a prevalence of 10-25% among GERD patients in Western populations, though rates vary by diagnostic criteria and endoscopy practices.[17] Eosinophilic esophagitis (EoE), an allergic subtype, has a rising prevalence in Western countries, estimated at approximately 140 cases per 100,000 individuals in the U.S. as of 2024 based on large-scale studies, equating to about 1 in 700 people.[18] Incidence trends for EoE demonstrate a marked increase over recent decades, with annual rates rising from 0.01 per 100,000 in 1995 to 3.16 per 100,000 by 2019 in population-based cohorts, largely due to heightened diagnostic awareness and improved endoscopic detection.[19] In children, EoE incidence reaches up to 10 per 100,000 in some regions, contributing to overall prevalence estimates of 24% among those with esophageal biopsies showing histological disease.[20] For reflux esophagitis, incidence remains relatively stable despite rising GERD prevalence, with erosive changes observed in about 28.7% of pediatric cases undergoing endoscopy, though adult rates have not shown similar escalation due to widespread use of proton pump inhibitors.[21] Geographically, EoE prevalence is higher in developed Western nations, such as the United States and Europe, where rates approach 1 per 1,000 in select populations, compared to much lower figures in Asia (around 1 per 5,000 endoscopies).[22] Infectious esophagitis, including candidal and viral forms, is more prevalent in immunocompromised individuals, affecting up to one-third of untreated AIDS patients, and is disproportionately common in low-resource settings with elevated HIV and immunosuppression rates.[23] [24] Demographically, EoE exhibits a strong male predominance with a 3:1 male-to-female ratio and peaks in incidence among young adults aged 20-40 years, with mean diagnosis age around 33-38 years.[25] [26] In contrast, reflux esophagitis increases with age, showing severe erosive disease in 37% of patients over 70 years compared to only 12% under 21, and is more common in older females post-50.[21] [27]Risk factors
Several factors increase the susceptibility to esophagitis, with risks varying by type. For reflux esophagitis, the most common form, key predisposing elements include obesity, which elevates intra-abdominal pressure and promotes gastroesophageal reflux; smoking, which relaxes the lower esophageal sphincter and impairs mucosal defenses; hiatal hernia, which disrupts the antireflux barrier at the gastroesophageal junction; and delayed gastric emptying, which prolongs exposure of the esophagus to refluxed contents.[28][6][3][29] Infectious esophagitis is particularly associated with immunocompromised states, such as HIV infection, chemotherapy, or use of immunosuppressive medications like steroids, which impair the body's ability to combat esophageal pathogens; diabetes also heightens risk by altering immune responses and mucosal integrity.[1][30][24] For eosinophilic esophagitis (EoE), an allergic-mediated type, individuals with a history of atopy—such as asthma, food allergies, or eczema—are at greater risk due to underlying immune dysregulation that promotes eosinophilic infiltration.[31][32][33] Pill-induced esophagitis arises from medications like nonsteroidal anti-inflammatory drugs (NSAIDs), bisphosphonates, and certain antibiotics, especially when taken without sufficient water, in a recumbent position, or immediately before lying down, leading to direct mucosal contact and erosion.[34][1][35] Environmental exposures, including radiation therapy to the chest, damage esophageal epithelium and increase vulnerability to inflammation.[3][36] Dietary factors such as frequent consumption of spicy foods, alcohol, or caffeine can exacerbate esophagitis by irritating the esophageal lining or stimulating acid production, particularly in those already predisposed.[6][4]Classification
Major types
Esophagitis is broadly classified into several major types based on underlying etiology and clinical presentation, with reflux esophagitis being the most prevalent form worldwide.[3] This classification helps distinguish between conditions that primarily involve acid exposure, infectious agents, immune responses, or direct mucosal injury, though overlaps can occur in clinical practice.[24] Reflux esophagitis arises from repeated exposure of the esophageal mucosa to gastric contents, resulting in inflammation, erosions, and potential ulceration along the distal esophagus.[3] It is characterized by symptoms such as heartburn and regurgitation, often linked to impaired lower esophageal sphincter function.[24] Infectious esophagitis encompasses microbial invasions of the esophageal lining, predominantly affecting immunocompromised individuals but also occurring in others with predisposing factors.[3] Candidal esophagitis, the most frequent subtype, features superficial plaques and white exudates due to overgrowth of Candida species on the mucosal surface.[3] Viral forms include herpes simplex virus (HSV)-associated esophagitis, marked by small vesicles that evolve into shallow ulcers, and cytomegalovirus (CMV) esophagitis, which produces larger, linear ulcers in the mid-to-distal esophagus.[24] Bacterial esophagitis remains rare, typically presenting with deeper ulcers from opportunistic pathogens.[3] Eosinophilic esophagitis (EoE) is a chronic, immune-mediated condition characterized by dense eosinophilic infiltration of the esophageal mucosa, often exceeding 15 eosinophils per high-power field in affected areas.[37] It is associated with allergic responses and manifests with esophageal dysfunction, including rings, furrows, or strictures visible on examination.[37] Other notable types include pill-induced esophagitis, which involves localized mucosal damage from direct contact with certain medications, leading to discrete ulcers at sites of pill retention.[3] Radiation-induced esophagitis occurs following therapeutic radiation exposure, presenting with acute mucosal erythema, edema, and friability, or chronic fibrosis and strictures.[24] Caustic esophagitis results from ingestion of corrosive substances, causing immediate chemical burns and layered necrosis of the esophageal wall.[24] Lymphocytic esophagitis is defined by prominent intraepithelial lymphocytic infiltration with spongiosis and minimal granulocytes, distinguishing it from other inflammatory patterns.[38] Sloughing esophagitis, also known as esophagitis dissecans superficialis, is a benign entity featuring superficial detachment and shedding of large mucosal sheets, often appearing as vertical strips on endoscopy.[39] Overlaps and mixed forms of esophagitis are common, particularly in patients with multiple risk factors, such as concurrent reflux and eosinophilic features or infectious complications superimposed on reflux esophagitis.[3] These hybrid presentations may require careful differentiation, with severity varying by dominant type.[24]Severity assessment
Severity assessment in esophagitis involves standardized systems to evaluate the extent and intensity of esophageal inflammation, aiding in clinical decision-making across different etiologies.[40] General metrics classify severity descriptively based on endoscopic appearance: mild esophagitis features erythema and edema without breaks in the mucosa; moderate involves superficial erosions or friability; and severe includes deep ulcers, confluent erosions, or complications like strictures.[41] These assessments help guide therapy escalation, such as initiating proton pump inhibitors for mild cases or considering advanced interventions for severe disease, and predict outcomes like response to treatment.[40][42] For reflux esophagitis, the Los Angeles (LA) classification is the most widely adopted endoscopic grading system, categorizing severity into grades A through D based on the number, length, and circumferential extent of mucosal breaks.[43] Grade A denotes one or more mucosal breaks less than 5 mm in length that do not extend between the tops of two mucosal folds; Grade B includes one or more breaks longer than 5 mm but confined to a single mucosal fold; Grade C features breaks extending over multiple folds involving less than 75% of the esophageal circumference; and Grade D involves breaks covering 75% or more of the circumference.[44] This system standardizes evaluation, facilitating consistent reporting and correlation with symptom severity and healing rates under therapy.[45] In eosinophilic esophagitis (EoE), severity is assessed through both histologic and endoscopic criteria. Histologically, active disease is defined by at least 15 eosinophils per high-power field (HPF) in esophageal biopsies, with higher counts indicating greater intensity of inflammation.[46] Endoscopically, the Eosinophilic Esophagitis Endoscopic Reference Score (EREFS) quantifies features such as rings, exudates, furrows, edema, and strictures, each scored from 0 to 3 based on prominence and extent, yielding a total score that reflects overall mucosal involvement.[47] These tools enable monitoring of treatment response, with reductions in eosinophil counts and EREFS scores predicting sustained remission and reduced risk of fibrosis.[48]Causes and pathophysiology
Etiology by type
Reflux esophagitis arises primarily from the backflow of gastric acid into the esophagus due to dysfunction of the lower esophageal sphincter (LES), which normally prevents such reflux.[28] This dysfunction often involves transient LES relaxations, allowing stomach acid, peptic enzymes, and sometimes bile to enter the esophagus.[49] Hiatal hernia can exacerbate this by promoting LES incompetence, though it is not the sole cause.[50] Infectious esophagitis is most commonly caused by opportunistic pathogens in immunocompromised individuals, with Candida species, particularly Candida albicans, accounting for up to 88% of cases and presenting as thrush-like plaques.[51] Herpes simplex virus (HSV) and cytomegalovirus (CMV) are key viral etiologies, often featuring viral inclusions in esophageal biopsies from affected patients; HSV typically causes small, superficial ulcers, while CMV leads to larger, linear ulcers.[52] Immunosuppression, such as in HIV or transplant recipients, amplifies susceptibility to these infections.[53] Eosinophilic esophagitis (EoE) is triggered by food allergens, such as milk, wheat, egg, soy, and peanut, which provoke a type 2 helper T (Th2) immune response characterized by elevated cytokines like IL-5 and IL-13.[54] Aeroallergens also contribute, potentially through epicutaneous exposure leading to systemic Th2 sensitization that affects the esophagus.[55] This allergic cascade is distinct from IgE-mediated reactions but shares atopic underpinnings.[56] Pill-induced esophagitis results from direct mucosal contact with certain medications, most notably doxycycline and other tetracyclines, among the most common causes due to their caustic properties when lodged in the esophagus.[34] Potassium chloride tablets are another frequent culprit, causing severe ulceration through prolonged local exposure, sometimes leading to strictures.[57] Nonsteroidal anti-inflammatory drugs and bisphosphonates can similarly provoke injury via chemical irritation.[58] Radiation esophagitis stems from exposure to ionizing radiation during therapy for thoracic malignancies, such as lung or esophageal cancer, where the esophageal mucosa absorbs doses that induce acute inflammation.[59] This damage occurs through direct DNA strand breaks in esophageal cells from the radiation beam.[60] Caustic esophagitis is induced by ingestion of corrosive chemicals, particularly alkaline agents like lye (sodium hydroxide), which cause immediate chemical burns and coagulation necrosis in the esophageal lining.[61] Acidic substances, such as battery acid, can also trigger similar injuries, though alkaline ingestions more commonly affect the esophagus due to their liquefying action on tissues.[62] Emerging etiologies include lymphocytic esophagitis, potentially linked to autoimmune mechanisms, as evidenced by associations with conditions like Crohn's disease and a predominance of intraepithelial lymphocytes without eosinophilic involvement.[38] Hypersensitivity reactions to ingestants or chronic inflammatory states may contribute, though the precise triggers remain unclear.[63]Mechanisms of inflammation
The mechanisms of inflammation in esophagitis involve a cascade of epithelial injury, immune cell activation, and tissue remodeling, varying by underlying etiology but converging on disruption of the mucosal barrier and cytokine-mediated responses.[3] In gastroesophageal reflux disease (GERD)-associated esophagitis, hydrochloric acid and pepsin from refluxed gastric contents directly erode the esophageal squamous epithelium, compromising the protective mucosal barrier and exposing subepithelial layers to further damage.[64] This erosion stimulates esophageal epithelial cells to secrete pro-inflammatory cytokines, including interleukin-8 (IL-8) and interleukin-1β (IL-1β), which recruit neutrophils and amplify the local inflammatory response.[65] IL-8, in particular, promotes neutrophil chemotaxis and activation, contributing to acute mucosal inflammation and edema.[66] Eosinophilic esophagitis (EoE) features a type 2 immune-mediated inflammation driven by allergen-triggered T helper 2 (Th2) cell activation, leading to eosinophil recruitment and chronic tissue changes.[3] Mast cells also play a key role by degranulating to release mediators that amplify the Th2 response and promote eosinophil activation.[67] Cytokines such as IL-5 and IL-13 play central roles: IL-5 promotes eosinophil maturation, survival, and migration into the esophageal mucosa, while IL-13 induces barrier dysfunction by downregulating tight junction proteins like filaggrin and claudins.[68] Additionally, transforming growth factor-β (TGF-β), released by eosinophils and epithelial cells, drives subepithelial fibrosis through extracellular matrix deposition and epithelial-mesenchymal transition, resulting in esophageal stricturing over time.[69] Infectious esophagitis, such as that caused by Candida species, involves fungal hyphae penetration of the compromised esophageal mucosa, particularly in immunocompromised hosts, leading to invasive tissue damage and secondary inflammation.[70] Candida albicans hyphae adhere to and invade epithelial cells via adhesins and hydrolytic enzymes, disrupting the barrier and eliciting a neutrophilic and mononuclear inflammatory response.[70] For herpes simplex virus (HSV)-induced esophagitis, viral replication within squamous epithelial cells produces cytopathic effects, including multinucleated giant cells and intranuclear inclusions, which cause cell lysis and ulceration, triggering localized acute inflammation.[71] Direct toxicity in pill-induced esophagitis occurs when medications, such as doxycycline or bisphosphonates, form crystalline aggregates or hyperosmolar solutions that contact the esophageal mucosa, causing localized chemical injury and necrosis.[34] This direct irritant effect erodes the epithelium and disrupts cytoprotective mucus layers, leading to focal inflammation and potential ulceration at sites of stasis, like the mid-esophagus.[72] In radiation esophagitis, ionizing radiation generates reactive oxygen species (ROS) that induce oxidative stress, damaging DNA and proteins in esophageal cells, which activates apoptotic pathways and proinflammatory cytokine release.[73] Across esophagitis subtypes, common inflammatory pathways include epithelial hyperplasia, where basal cell proliferation compensates for injury, often driven by cytokines like IL-13 and leading to thickened mucosa.[3] Angiogenesis, mediated by vascular endothelial growth factor (VEGF) from inflamed tissues, supports neovascularization to sustain chronic inflammation.[74] Extracellular matrix (ECM) remodeling, involving collagen deposition and matrix metalloproteinase activity, contributes to fibrosis and stiffness, particularly in chronic forms like EoE and reflux esophagitis.[75]Diagnosis
Clinical evaluation
The clinical evaluation of esophagitis begins with a detailed history-taking to identify symptoms suggestive of esophageal inflammation and to assess for potential underlying causes or complications. Patients often report dysphagia, characterized by difficulty swallowing solids or liquids, which may have a gradual onset in chronic forms like gastroesophageal reflux disease (GERD)-related esophagitis or abrupt in acute cases such as infectious or pill-induced esophagitis. Odynophagia, or painful swallowing, is another key symptom, frequently linked to erosive damage from acid exposure or infection. Clinicians inquire about the duration of symptoms, their relation to meals—such as worsening heartburn or regurgitation postprandially in reflux esophagitis—and associated features like chronic cough or wheezing, which may indicate extraesophageal reflux. Alarm symptoms, including unintentional weight loss, hematemesis (vomiting blood), or melena (black, tarry stools), warrant urgent evaluation to rule out severe complications like ulceration or bleeding.[3][1][2] The physical examination in esophagitis is typically unremarkable and plays a supportive rather than diagnostic role, as direct signs of esophageal involvement are rare. Indirect findings may include signs of dehydration, such as dry mucous membranes or reduced skin turgor, in patients with severe odynophagia leading to reduced oral intake. In cases of infectious esophagitis, particularly candidal esophagitis in immunocompromised individuals, oral thrush—manifesting as white plaques on the buccal mucosa or tongue—may be observed and suggests possible esophageal extension. Tenderness to palpation over the suprasternal notch or epigastrium can occasionally occur in severe inflammation but is nonspecific. Overall, the physical exam helps gauge the patient's nutritional status and general well-being but rarely confirms the diagnosis independently.[3][1] Red flags identified during history and exam prompt immediate intervention to prevent life-threatening issues. Acute onset of severe retrosternal pain, especially following caustic ingestion (e.g., accidental or intentional exposure to corrosive substances), raises concern for chemical injury, perforation, or mediastinitis, necessitating emergent assessment. Similarly, sudden food impaction with intractable vomiting or hematemesis signals possible Boerhaave syndrome or esophageal rupture. These features guide triage, with patients exhibiting such urgency transferred to specialized care for rapid stabilization.[3][1][2] A critical aspect of clinical evaluation is differentiating esophagitis from mimics to avoid misdiagnosis and inappropriate management. For instance, retrosternal pain and dysphagia may overlap with cardiac conditions like acute coronary syndrome, particularly in older adults; history details such as exertional onset versus meal-related triggers, absence of radiation to the arm or jaw, and lack of diaphoresis help distinguish esophageal from ischemic pain. Other mimics include musculoskeletal chest wall pain or pharyngeal disorders, where the absence of odynophagia or regurgitation points away from esophagitis. This initial assessment establishes suspicion for esophagitis while highlighting the need for further targeted investigation in ambiguous cases.[3][2]Endoscopic and biopsy findings
Endoscopy plays a central role in the diagnosis of esophagitis by providing direct visualization of mucosal abnormalities, which vary by etiology and guide biopsy site selection.[3] In reflux esophagitis, common findings include mucosal erythema, friability, and erosions, often graded using the Los Angeles (LA) classification system: grade A features one or more mucosal breaks no longer than 5 mm that do not extend between the tops of two mucosal folds; grade B includes one or more mucosal breaks longer than 5 mm that do not extend between the tops of two mucosal folds; grade C involves mucosal breaks that are continuous and extend between the tops of two or more mucosal folds; and grade D encompasses one or more mucosal breaks involving at least 75% of the esophageal circumference.[76] For eosinophilic esophagitis (EoE), endoscopic features typically manifest as linear furrows, trachealization (rings), white exudates, edema, and strictures, systematically assessed via the Eosinophilic Esophagitis Endoscopic Reference Score (EREFS), which grades each feature from 0 to 3 (edema, rings, exudates, strictures) or 0 to 2 (furrows) for a total score reflecting disease severity.[47] Infectious esophagitis presents with distinct patterns: candidal esophagitis shows adherent yellow-white plaques; herpes simplex virus (HSV) esophagitis features multiple small, superficial, punched-out ulcers often with a volcanic appearance; and cytomegalovirus (CMV) esophagitis displays larger, shallow, linear or serpiginous ulcers, typically in the mid-to-distal esophagus.[3] Biopsy findings provide histopathological confirmation and differentiation among esophagitis types. In reflux esophagitis, biopsies reveal basal cell hyperplasia (with >15% of the epithelial thickness occupied by basal cells), elongation of lamina propria papillae up to the upper third of the epithelium, and variable inflammatory infiltrates including neutrophils, eosinophils, and intracellular edema.[77] EoE is characterized by dense eosinophilic infiltration, with at least 15 eosinophils per high-power field (HPF) in the esophageal squamous epithelium, often forming eosinophilic microabscesses, alongside surface layering of eosinophils, basal zone expansion, and lamina propria fibrosis; diagnosis requires symptoms of esophageal dysfunction, this histologic finding, and exclusion of secondary causes per current guidelines.[78][79] For infectious causes, candidal biopsies demonstrate pseudohyphae and yeast forms invading the superficial epithelium with associated acute inflammation; HSV shows multinucleated giant cells, ground-glass nuclei, and Cowdry or Bead-like intranuclear inclusions in squamous cells at ulcer edges; and CMV exhibits enlarged cells with cytomegalic changes, including basophilic cytoplasmic and eosinophilic nuclear (owl's eye) inclusions in endothelial or stromal cells.[3] Appropriate sampling techniques enhance diagnostic yield, involving multiple biopsies (typically 4-6 samples) from both proximal and distal esophagus, including from normal-appearing and abnormal mucosa, to account for patchy involvement and increase sensitivity for conditions like EoE.[80] These endoscopic and biopsy findings not only confirm the specific type of esophagitis but also play a crucial role in excluding mimics such as malignancy, pill-induced injury, or other inflammatory disorders through targeted tissue analysis.[3] Endoscopic grading systems like LA and EREFS further inform severity assessment, correlating with clinical outcomes.[76]Additional tests
In cases of suspected esophagitis, particularly gastroesophageal reflux disease (GERD)-related, pH-impedance monitoring serves as a key functional test to confirm pathologic reflux and quantify acid exposure beyond endoscopic findings. This ambulatory test involves placing a catheter through the nose into the esophagus to measure pH levels and impedance over 24 hours, detecting both acid and non-acid reflux events while correlating them with symptoms. Abnormal results per Lyon Consensus include acid exposure time >6% of the total monitoring period (pH <4) as pathologic, 4-6% inconclusive; upright (daytime) exposure exceeding 6.3% may support pathology in many guidelines, helping differentiate reflux esophagitis from other etiologies.[81][49] Barium swallow radiography, also known as esophagogram, provides a non-invasive imaging modality to evaluate structural abnormalities in esophagitis, such as strictures, rings, or motility disturbances that may contribute to symptoms like dysphagia. During the procedure, the patient swallows barium contrast under fluoroscopy, allowing visualization of esophageal contour, narrowing, or irregular contractions indicative of chronic inflammation or fibrosis. It is particularly useful for detecting peptic strictures in reflux esophagitis or diffuse narrowing in eosinophilic esophagitis (EoE), though it should be avoided in suspected esophageal perforation due to the risk of barium extravasation causing mediastinitis.[82][83] For EoE, where food allergens often trigger eosinophilic inflammation, allergy testing via skin prick or atopy patch testing identifies potential dietary triggers among common foods such as milk, wheat, eggs, and soy. Skin prick testing involves applying allergen extracts to the skin and pricking to detect IgE-mediated reactions, while patch testing assesses delayed hypersensitivity by applying allergens under occlusive patches for 48 hours, followed by reading for reactions. These tests guide empiric elimination diets, with positive results in up to 70% of pediatric and 50-60% of adult EoE cases, though negative predictive value is high for most foods except milk.[84][85] Esophageal manometry assesses motility disorders associated with esophagitis-related strictures or fibrosis, measuring pressure and coordination of esophageal contractions during swallows. High-resolution manometry, using multiple sensors along a transnasal catheter, detects abnormalities like ineffective esophageal motility or nutcracker esophagus, which occur in about one-third of EoE patients and can exacerbate stricture symptoms. It is indicated when dysphagia persists despite treatment, helping evaluate lower esophageal sphincter function and peristalsis integrity in fibrostenotic esophagitis.[86][87] Blood tests support the diagnostic workup by identifying peripheral eosinophilia or infectious causes in esophagitis. Elevated absolute eosinophil counts (>500 cells/mm³ or >5% of white blood cells) suggest allergic or EoE-related inflammation, though not diagnostic alone as they occur in 5-50% of cases. Serologic testing for antibodies against pathogens like herpes simplex virus or Candida is useful in infectious esophagitis, particularly in immunocompromised patients, to confirm etiology when biopsy is inconclusive.[88][89]Management
Prevention strategies
Preventing esophagitis involves targeted strategies to mitigate risk factors associated with its major types, including gastroesophageal reflux disease (GERD)-related, infectious, and eosinophilic forms, as well as general measures against caustic injury. For GERD-associated esophagitis, lifestyle interventions form the cornerstone of prevention, particularly in at-risk populations such as obese individuals and smokers. Weight management through sustained loss to achieve a BMI below 25 has been shown to reduce reflux episodes by decreasing intra-abdominal pressure and improving lower esophageal sphincter function.[90] Smoking cessation is equally critical, as tobacco weakens the lower esophageal sphincter and delays gastric emptying, thereby diminishing reflux risk upon quitting; limiting alcohol intake further supports this.[91] Additionally, elevating the head of the bed by 15-20 cm during sleep prevents nocturnal acid reflux by leveraging gravity to keep gastric contents below the esophagogastric junction; avoiding tight clothing around the abdomen also reduces pressure on the sphincter.[92] Infectious esophagitis, often seen in immunocompromised patients, can be prevented through prophylactic measures tailored to high-risk groups like solid organ transplant recipients. Antifungal prophylaxis, such as with systemic triazoles or nebulized amphotericin, is routinely employed in lung transplant patients for the first six months post-transplant to avert candidal esophagitis, given the elevated incidence in this cohort.[93] For herpetic esophagitis due to herpes simplex virus (HSV) in immunocompromised individuals, antiviral prophylaxis with acyclovir or valacyclovir is recommended in cases of frequent recurrences or high exposure risk, though routine primary prophylaxis is not standard; no commercial HSV vaccine is currently available for prevention.[94] Pill-induced esophagitis, a non-infectious form, is avoided by instructing patients to swallow medications with at least 8 ounces of water and remain upright for 30 minutes afterward, which facilitates passage through the esophagus and reduces mucosal contact time; if a pill becomes stuck causing pain, drinking more water can help relieve symptoms by flushing or sliding the pill down into the stomach and reducing esophageal irritation or inflammation; discontinuing or switching offending agents like aspirin or NSAIDs is key for drug-induced cases.[34] Eosinophilic esophagitis (EoE) prevention emphasizes early intervention in at-risk families, particularly those with a history of atopic diseases or food allergies. Dietary strategies involving proactive avoidance of common triggers like milk, wheat, egg, and soy may help reduce disease onset in genetically predisposed children, though evidence is primarily derived from management studies showing allergen elimination's efficacy in halting progression.[95] Public health initiatives play a vital role here, with awareness campaigns promoting symptom recognition—such as dysphagia and food impaction—to facilitate earlier diagnosis amid rising EoE incidence, as seen in efforts by organizations like the American Partnership for Eosinophilic Disorders.[96] Broader preventive approaches address caustic esophagitis through community-level actions. Avoiding ingestion of household chemicals like drain cleaners or batteries is essential, supported by public education programs that emphasize secure storage, childproof packaging, and poison control awareness to curb accidental exposures, which disproportionately affect children.[61] These multifaceted strategies, combining individual behaviors and societal interventions, underscore the importance of tailored prevention to lower esophagitis burden across populations.Lifestyle modifications
Lifestyle modifications play a crucial role in managing active esophagitis by reducing esophageal irritation, alleviating symptoms such as heartburn and dysphagia, and supporting mucosal healing without relying on medications. These changes are tailored to the underlying type of esophagitis and focus on dietary, positional, and habitual adjustments that patients can implement daily under medical guidance.[97] Dietary adjustments are foundational, emphasizing the avoidance of irritants and optimization of meal patterns to minimize reflux or allergic triggers. For reflux-related esophagitis, patients should avoid common triggers such as spicy, oily, or acidic foods, caffeine, chocolate, alcohol, carbonated drinks, and mint-flavored foods, while opting for smaller, more frequent meals to reduce gastric pressure and acid exposure; no eating should occur at least three hours before bedtime. In eosinophilic esophagitis (EoE), elimination diets are particularly effective; the six-food elimination diet, which excludes milk, wheat, eggs, soy, nuts, and fish/seafood, has been shown to induce remission in a significant proportion of cases by targeting food allergens. Chewing food thoroughly and consuming meals slowly further aids digestion and prevents bolus impaction, especially in EoE where patients often develop compensatory eating behaviors.[98][99][100][88][101] Positional changes help prevent acid reflux and promote esophageal clearance. Remaining upright for at least three hours after meals reduces the likelihood of gastric contents entering the esophagus, while elevating the head of the bed by 15-20 cm using a wedge or blocks—rather than stacked pillows—can decrease nighttime symptoms in reflux esophagitis. Avoiding bending or stooping immediately after eating further supports these efforts.[97][98] Habit modifications address broader risk factors and mechanical stressors. Achieving a 5-10% reduction in body weight through diet and exercise has been associated with significant improvement in GERD symptoms and reduced esophageal acid exposure, particularly beneficial for overweight individuals with reflux esophagitis. Smoking cessation is essential, as it impairs lower esophageal sphincter function and exacerbates inflammation. For pill-induced esophagitis, specific habits include taking medications with at least 200-250 ml of water, remaining upright for 30 minutes afterward, and avoiding bedtime dosing to prevent direct mucosal contact. Consuming soft foods and emphasizing hydration can minimize further irritation in this type, while steering clear of hot, cold, or acidic items promotes comfort during recovery.[102][97][34][34]Pharmacological treatments
Pharmacological treatments for esophagitis are etiology-specific, targeting acid suppression, infection, inflammation, or mucosal protection to promote healing and symptom relief. For reflux esophagitis, proton pump inhibitors (PPIs) such as omeprazole, lansoprazole, rabeprazole, pantoprazole, or esomeprazole at 1-2 times daily for 4-8 weeks are first-line, suppressing gastric acid production and achieving endoscopic healing rates of 80-90% after 8 weeks in patients with Los Angeles (LA) grades A-B disease; H2 blockers like famotidine are suitable for mild cases, while antacids such as aluminum hydroxide or calcium carbonate provide quick relief for heartburn. Prokinetics like domperidone or mosapride may serve as adjuncts to aid gastric emptying in select patients with delayed motility.[103][104] Infectious esophagitis requires antimicrobial therapy, including antibiotics, antifungals, or antivirals tailored to the pathogen; for candidal esophagitis, oral fluconazole at 200 mg daily for 14-21 days eradicates the fungus in most cases by inhibiting ergosterol synthesis in fungal cell membranes.[105] For herpes simplex virus (HSV) esophagitis, acyclovir at 5 mg/kg intravenously every 8 hours or 400 mg orally five times daily for 7-14 days inhibits viral DNA polymerase, leading to rapid symptom resolution in immunocompetent patients.[106][107] Eosinophilic esophagitis (EoE) management emphasizes anti-inflammatory agents, with high-dose PPIs (e.g., omeprazole 40 mg BID) suggested as an initial treatment option per the 2025 American College of Gastroenterology (ACG) guidelines, with up to 50% of cases showing reduced eosinophilic infiltration; topical or oral steroids are also used alongside allergen elimination.[108] The guidelines strongly recommend swallowed topical corticosteroids such as budesonide slurry (2 mg twice daily, mixed for esophageal coating) or oral suspension (2 mg twice daily for ages 11 and older; FDA-approved February 2024) to induce histologic remission by locally suppressing Th2-mediated inflammation.[109][110] Biologics like dupilumab (300 mg subcutaneously weekly in adults, FDA-approved in January 2024; also approved for children aged 1-11 years weighing at least 15 kg) target IL-4 and IL-13 pathways, yielding histologic response rates over 60% in clinical trials.[111][112] For pill-induced esophagitis, discontinuing offending drugs like aspirin or NSAIDs is primary, with sucralfate at 1 g orally four times daily forming a protective barrier over eroded mucosa to aid healing without systemic absorption.[34] Symptomatic pain relief across types may involve viscous lidocaine (2% solution, 15 mL gargled and swallowed every 3 hours as needed), providing local anesthesia to the esophageal lining.[113] Long-term PPI use necessitates monitoring for hypomagnesemia, which can occur after months of therapy due to impaired intestinal absorption and manifest as fatigue or arrhythmias.[114] In EoE, treatment efficacy is assessed by histologic remission criteria of fewer than 15 eosinophils per high-power field (eos/HPF) on biopsy.[115]Complementary and alternative approaches
No complementary or alternative medicines are proven to treat esophagitis definitively. However, some herbal remedies and supplements may help ease symptoms such as heartburn or irritation in cases of reflux esophagitis, based on preliminary clinical studies, reviews, and traditional use. These should not replace conventional treatments like proton pump inhibitors (PPIs) and must be discussed with a healthcare professional to avoid interactions or risks. Commonly mentioned options include:- Slippery elm bark: Forms a protective gel-like coating on the esophageal lining, potentially soothing irritation.
- Aloe vera juice/syrup: Anti-inflammatory properties; small studies suggest reduction in heartburn, regurgitation, and mucosal damage in GERD.
- Deglycyrrhizinated licorice (DGL): May promote mucus production and protect/heal the esophageal lining; evidence for GERD symptom relief.
- Zinc carnosine: Adheres to inflamed areas, supporting mucosal repair.
- L-Glutamine: Amino acid that may aid repair of damaged gastrointestinal lining.
- Melatonin: Some studies indicate protective effects on esophageal mucosa and potential superiority to PPIs in combination for symptom relief.
- Probiotics: Certain strains (e.g., Lactobacillus, Bifidobacterium) may reduce reflux symptoms and support gut balance.
- Ginger: Anti-inflammatory; may alleviate irritation but can relax LES in some cases.
- Chamomile: Soothing anti-inflammatory effects for esophageal irritation.