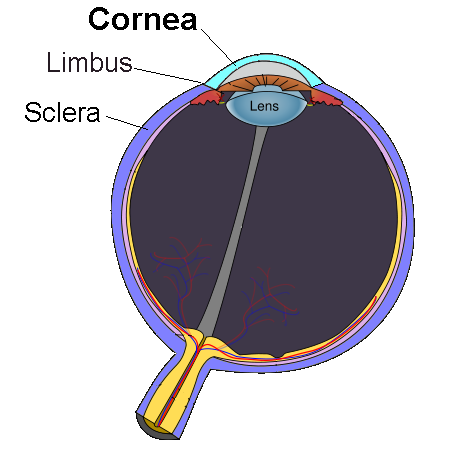
The cornea is the transparent front part of the eyeball which covers the iris, pupil, and anterior chamber. Along with the anterior chamber and lens, the cornea refracts light, accounting for approximately two-thirds of the eye's total optical power.[1][2] In humans, the refractive power of the cornea is approximately 43 dioptres.[3] The cornea can be reshaped by surgical procedures such as LASIK.[4]
While the cornea contributes most of the eye's focusing power, its focus is fixed. Accommodation (the refocusing of light to better view near objects) is accomplished by changing the geometry of the lens. Medical terms related to the cornea often start with the prefix "kerat-" from the Greek word κέρας, horn.
The cornea has unmyelinatednerve endings sensitive to touch, temperature and chemicals; a touch of the cornea causes an involuntary reflex to close the eyelid. Because transparency is of prime importance, the healthy cornea does not have or need blood vessels within it. Instead, oxygen dissolves in tears and then diffuses throughout the cornea to keep it healthy.[5] Similarly, nutrients are transported via diffusion from the tear fluid through the outside surface and the aqueous humour through the inside surface. Nutrients also come via neurotrophins supplied by the nerves of the cornea. In humans, the cornea has a diameter of about 11.5 mm and a thickness of 0.5–0.6 mm in the center and 0.6–0.8 mm at the periphery. Transparency, avascularity, the presence of immature resident immune cells, and immunologic privilege makes the cornea a very special tissue.
The most abundant soluble protein in mammalian cornea is albumin.[6]
The human cornea borders with the sclera at the corneal limbus. In lampreys, the cornea is solely an extension of the sclera, and is separate from the skin above it, but in more advanced vertebrates it is always fused with the skin to form a single structure, albeit one composed of multiple layers. In fish, and aquatic vertebrates in general, the cornea plays no role in focusing light, since it has virtually the same refractive index as water.[7]
Vertical section of human cornea from near the margin. (Waldeyer.) Magnified. 1: Epithelium. 2: Anterior elastic lamina. 3: substantia propria. 4: Posterior elastic lamina (Descemet's membrane). 5: Endothelium of the anterior chamber. a: Oblique fibers in the anterior layer of the substantia propria. b: Lamellae, the fibers of which are cut across, producing a dotted appearance. c: Corneal corpuscles appearing fusiform in section. d: Lamellae, the fibers of which are cut longitudinally. e: Transition to the sclera, with more distinct fibrillation, and surmounted by a thicker epithelium. f: Small blood vessels cut across near the margin of the cornea.Corneal cross-section imaged by an SD-OCT
The human cornea has five layers (possibly six, if the Dua's layer is included).[8] Corneas of other primates have five known layers. The corneas of cats, dogs, wolves, and other carnivores only have four.[9] From the anterior to posterior the layers of the human cornea are:
Corneal epithelium: an exceedingly thin multicellular epithelial tissue layer (non-keratinized stratified squamous epithelium) of fast-growing and easily regenerated cells, kept moist with tears. Irregularity or edema of the corneal epithelium disrupts the smoothness of the air/tear-film interface, the most significant component of the total refractive power of the eye, thereby reducing visual acuity. Corneal epithelium is continuous with the conjunctival epithelium, and is composed of about 6 layers of cells which are shed constantly on the exposed layer and are regenerated by multiplication in the basal layer.
Bowman's layer (also known as the anterior limiting membrane): when discussed in lieu of a subepithelial basement membrane, Bowman's Layer is a tough layer composed of collagen (mainly type I collagen fibrils), laminin, nidogen, perlecan and other HSPGs that protects the corneal stroma. When discussed as a separate entity from the subepithelial basement membrane, Bowman's Layer can be described as an acellular, condensed region of the apical stroma, composed primarily of randomly organized yet tightly woven collagen fibrils. These fibrils interact with and attach onto each other. This layer is eight to 14 micrometres (μm) thick[10] and is absent or very thin in non-primates.[9][11]
Corneal stroma (also substantia propria): a thick, transparent middle layer, consisting of regularly arranged collagen fibers along with sparsely distributed interconnected keratocytes, which are the cells for general repair and maintenance.[10] They are parallel and are superimposed like book pages. The corneal stroma consists of approximately 200 layers of mainly type I collagen fibrils. Each layer is 1.5-2.5 μm. Up to 90% of the corneal thickness is composed of stroma.[10] There are 2 theories of how transparency in the cornea comes about:
The lattice arrangements of the collagen fibrils in the stroma. The light scatter by individual fibrils is cancelled by destructive interference from the scattered light from other individual fibrils.[12]
The spacing of the neighboring collagen fibrils in the stroma must be < 200 nm for there to be transparency. (Goldman and Benedek)
Descemet's membrane (also posterior limiting membrane): a thin acellular layer that serves as the modified basement membrane of the corneal endothelium, from which the cells are derived. This layer is composed mainly of collagen type IV fibrils, less rigid than collagen type I fibrils, and is around 5-20 μm thick, depending on the subject's age. Just anterior to Descemet's membrane, a very thin and strong layer, Dua's layer, 15 microns thick and able to withstand 1.5 to 2 bars of pressure.[13]
In a healthy eye, the cornea presents as a clear, domed, glossy covering over the iris and pupil.Corneal endothelium: a simple squamous or low cuboidal monolayer, approx 5 μm thick, of mitochondria-rich cells. These cells are responsible for regulating fluid and solute transport between the aqueous and corneal stromal compartments.[14] (The term endothelium is a misnomer here. The corneal endothelium is bathed by aqueous humor, not by blood or lymph, and has a very different origin, function, and appearance from vascular endothelia.) Unlike the corneal epithelium, the cells of the endothelium do not regenerate. Instead, they stretch to compensate for dead cells which reduces the overall cell density of the endothelium, which affects fluid regulation. If the endothelium can no longer maintain a proper fluid balance, stromal swelling due to excess fluids and subsequent loss of transparency will occur and this may cause corneal edema and interference with the transparency of the cornea and thus impairing the image formed.[14] Iris pigment cells deposited on the corneal endothelium can sometimes be washed into a distinct vertical pattern by the aqueous currents - this is known as Krukenberg's Spindle.
The cornea is one of the most sensitive tissues of the body, as it is densely innervated with sensory nerve fibres via the ophthalmic division of the trigeminal nerve by way of 70–80 long ciliary nerves. Research suggests the density of pain receptors in the cornea is 300–600 times greater than skin and 20–40 times greater than dental pulp,[15] making any injury to the structure excruciatingly painful.[16]
The ciliary nerves run under the endothelium and exit the eye through holes in the sclera apart from the optic nerve (which transmits only optic signals).[10] The nerves enter the cornea via three levels; scleral, episcleral and conjunctival. Most of the bundles give rise by subdivision to a network in the stroma, from which fibres supply the different regions. The three networks are, midstromal, subepithelial/sub-basal, and epithelial. The receptive fields of each nerve ending are very large, and may overlap.
Corneal nerves of the subepithelial layer terminate near the superficial epithelial layer of the cornea in a logarithmic spiral pattern.[17] The density of epithelial nerves decreases with age, especially after the seventh decade.[18]
The optical component is concerned with producing a reduced inverted image on the retina. The eye's optical system consists of not only two but four surfaces—two on the cornea, two on the lens. Rays are refracted toward the midline. Distant rays, due to their parallel nature, converge to a point on the retina. The cornea admits light at the greatest angle. The aqueous and vitreous humors both have a refractive index of 1.336-1.339, whereas the cornea has a refractive index of 1.376. Because the change in refractive index between cornea and aqueous humor is relatively small compared to the change at the air–cornea interface, it has a negligible refractive effect, typically -6 dioptres.[10] The cornea is considered to be a positive meniscus lens.[19] Some species of birds and chameleons, and one kinown species of fish, also have corneas which can focus.[20]
The cornea becomes opaque after death (provenance: genus Bos)
Upon death or removal of an eye the cornea absorbs the aqueous humor, thickens, and becomes hazy. Transparency can be restored by putting it in a warm, well-ventilated chamber at 31 °C (88 °F, the normal temperature), allowing the fluid to leave the cornea and become transparent. The cornea takes in fluid from the aqueous humor and the small blood vessels of the limbus, but a pump ejects the fluid immediately upon entry. When energy is deficient the pump may fail, or function too slowly to compensate, leading to swelling. This arises at death, but a dead eye can be placed in a warm chamber with a reservoir of sugar and glycogen that generally keeps the cornea transparent for at least 24 hours.[10]
The endothelium controls this pumping action, and as discussed above, damage thereof is more serious, and is a cause of opaqueness and swelling. When damage to the cornea occurs, such as in a viral infection, the collagen used to repair the process is not regularly arranged, leading to an opaque patch (leukoma).
The most common corneal disorders are the following:
Corneal abrasion – a medical condition involving the loss of the surface epithelial layer of the eye's cornea as a result of trauma to the surface of the eye.
Corneal dystrophy – a condition in which one or more parts of the cornea lose their normal clarity due to a buildup of cloudy material.
Corneal ulcer – an inflammatory or infective condition of the cornea involving disruption of its epithelial layer with involvement of the corneal stroma.
Corneal neovascularization – excessive ingrowth of blood vessels from the limbal vascular plexus into the cornea, caused by deprivation of oxygen from the air.
Various refractive eye surgery techniques change the shape of the cornea in order to reduce the need for corrective lenses or otherwise improve the refractive state of the eye. In many of the techniques used today, reshaping of the cornea is performed by photoablation using the excimer laser.
There are also synthetic corneas (keratoprostheses) in development. Most are merely plastic inserts, but there are also those composed of biocompatible synthetic materials that encourage tissue ingrowth into the synthetic cornea, thereby promoting biointegration. Other methods, such as magnetic deformable membranes[22] and optically coherent transcranial magnetic stimulation of the human retina[23] are still in very early stages of research.
Orthokeratology is a method using specialized hard or rigid gas-permeable contact lenses to transiently reshape the cornea in order to improve the refractive state of the eye or reduce the need for eyeglasses and contact lenses.
In 2009, researchers at the University of Pittsburgh Medical center demonstrated that stem cell collected from human corneas can restore transparency without provoking a rejection response in mice with corneal damage.[24] For corneal epithelial diseases such as Stevens Johnson Syndrome, persistent corneal ulcer etc., the autologous contralateral (normal) suprabasal limbus derived in vitro expanded corneal limbal stem cells are found to be effective[25] as amniotic membrane based expansion is controversial.[26] For endothelial diseases, such as bullous keratopathy, cadaver corneal endothelial precursor cells have been proven to be efficient. Recently emerging tissue engineering technologies are expected to be capable of making one cadaver-donor's corneal cells be expanded and be usable in more than one patient's eye.[27][28] One such technique has been reported to be safe and efficacious in a clinical pilot study with long term follow-up. [29]
Corneal retention and permeability in topical drug delivery to the eye
The majority of ocular therapeutic agents are administered to the eye via the topical route. Cornea is one of the main barriers for drug diffusion because of its highly impermeable nature. Its continuous irrigation with a tear fluid also results in poor retention of the therapeutic agents on the ocular surface. Poor permeability of the cornea and quick wash out of therapeutic agents from ocular surface result in very low bioavailability of the drugs administered via topical route (typically less than 5%). Poor retention of formulations on ocular surfaces could potentially be improved with the use of mucoadhesive polymers.[30] Drug permeability through the cornea could be facilitated with addition of penetration enhancers into topical formulations.[31]
If the corneal stroma develops visually significant opacity, irregularity, or edema, a cornea of a deceased donor can be transplanted. Because there are no blood vessels in the cornea, there are also few problems with rejection of the new cornea.
When a cornea is needed for transplant, as from an eye bank, the best procedure is to remove the cornea from the eyeball, preventing the cornea from absorbing the aqueous humor.[10]
There is a global shortage of corneal donations, severely limiting the availability of corneal transplants across most of the world. A 2016 study found that 12.7 million visually impaired people were in need of a corneal transplant, with only 1 cornea available for every 70 needed.[32] Many countries have years-long waitlists for corneal transplant surgery due to the shortage of donated corneas.[33][34] Only a handful of countries consistently have a large enough supply of donated corneas to meet local demand without a waitlist, including the United States, Italy, and Sri Lanka.[32]
^Hayashi, Shuichiro; Osawa, Tokuji; Tohyama, Koujiro (2002). "Comparative observations on corneas, with special reference to bowman's layer and descemet's membrane in mammals and amphibians". Journal of Morphology. 254 (3): 247–58. doi:10.1002/jmor.10030. PMID12386895. S2CID790199.
^Dua, Harminder S.; Faraj, Lana A.; Said, Dalia G.; Gray, Trevor; Lowe, James (2013). "Human Corneal Anatomy Redefined". Ophthalmology. 120 (9): 1778–85. doi:10.1016/j.ophtha.2013.01.018. PMID23714320.
^ abYanoff, Myron; Cameron, Douglas (2012). "Diseases of the Visual System". In Goldman, Lee; Schafer, Andrew I. (eds.). Goldman's Cecil Medicine (24th ed.). Elsevier Health Sciences. pp. 2426–42. ISBN978-1-4377-1604-7.
^Richter, Lars; Bruder, Ralf; Schlaefer, Alexander; Schweikard, Achim (2010). "Towards direct head navigation for robot-guided Transcranial Magnetic Stimulation using 3D laserscans: Idea, setup and feasibility". 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology. Vol. 2010. pp. 2283–86. doi:10.1109/IEMBS.2010.5627660. ISBN978-1-4244-4123-5. PMID21097016. S2CID3092563.
^Sitalakshmi, G.; Sudha, B.; Madhavan, H.N.; Vinay, S.; Krishnakumar, S.; Mori, Yuichi; Yoshioka, Hiroshi; Abraham, Samuel (2009). "Ex Vivo Cultivation of Corneal Limbal Epithelial Cells in a Thermoreversible Polymer (Mebiol Gel) and Their Transplantation in Rabbits: An Animal Model". Tissue Engineering Part A. 15 (2): 407–15. doi:10.1089/ten.tea.2008.0041. PMID18724830.
^Parikumar, Periyasamy; Haraguchi, Kazutoshi; Ohbayashi, Akira; Senthilkumar, Rajappa; Abraham, Samuel J. K. (2014). "Successful Transplantation of In Vitro Expanded Human Cadaver Corneal Endothelial Precursor Cells On to a Cadaver Bovine's Eye Using a Nanocomposite Gel Sheet". Current Eye Research. 39 (5): 522–6. doi:10.3109/02713683.2013.838633. PMID24144454. S2CID23131826.
^Ludwig, Annick (2005-11-03). "The use of mucoadhesive polymers in ocular drug delivery". Advanced Drug Delivery Reviews. Mucoadhesive Polymers: Strategies, Achievements and Future Challenges. 57 (11): 1595–1639. doi:10.1016/j.addr.2005.07.005. ISSN0169-409X. PMID16198021.
^ abGain P, Jullienne R, He Z, et al. Global Survey of Corneal Transplantation and Eye Banking. JAMA Ophthalmol. 2016;134(2):167–173. doi:10.1001/jamaophthalmol.2015.4776
^Kramer L. Corneal transplant wait list varies across Canada. CMAJ. 2013;185(11):E511-E512. doi:10.1503/cmaj.109-4517
^Hara H, Cooper DKC. Xenotransplantation: the future of corneal transplantation? Cornea. 2011;30(4):371-378. doi:10.1097/ICO.0b013e3181f237ef
The cornea is the transparent, dome-shaped anterior portion of the outer fibrous coat of the eye, covering the iris, pupil, and anterior chamber, and serving as the eye's primary optical interface by refracting light to focus images on the retina while acting as a protective barrier against external threats such as pathogens, trauma, and dehydration.[1] It is avascular, deriving its oxygen primarily from atmospheric air via tear film diffusion and nutrients from the aqueous humor, which enables its remarkable clarity essential for vision.[2]Structurally, the cornea measures approximately 11.7 mm horizontally and 10.6 mm vertically in adults, with a central thickness of about 0.5–0.6 mm, and consists of five primary layers that contribute to its mechanical strength, transparency, and refractive properties.[3] The outermost epithelium is a non-keratinized stratified squamous layer, 5–6 cells thick, that regenerates rapidly and forms a tight barrier to prevent entry of foreign substances, microbes, and fluid while allowing nutrient absorption.[4] Beneath it lies Bowman's layer, a thin, acellular collagenous sheet that provides structural support and resists swelling or scarring.[1] The stroma, comprising roughly 90% of the corneal thickness, is a dense, organized lattice of collagen fibrils arranged in lamellae, maintained by keratocytes, which ensures optical transparency through precise spacing that minimizes light scattering.[3] The posterior layers include Descemet's membrane, a resilient basement membrane secreted by the endothelium, and the single layer of endothelial cells, which actively pump ions and fluid from the stroma to the anterior chamber via Na+/K+-ATPase pumps, thereby regulating hydration and preserving deturgescence for clarity.[4] Some anatomical models recognize a sixth layer, Dua's layer, a distinct acellular band within the posterior stroma that enhances tensile strength.[5]Functionally, the cornea provides about two-thirds of the eye's total refractive power (approximately 43 diopters),[6] working in concert with the lens to converge light rays, and its smooth, curved surface minimizes aberrations for sharp vision.[7] It also contributes to the tear film stability, aiding in lubrication and further protection, while its dense innervation by the ophthalmic branch of the trigeminal nerve enables the corneal reflex to shield the eye from harm.[2] Transparency is maintained by the absence of blood vessels, regular stromal collagen alignment, and endothelial deturgescence, but disruptions can lead to opacity, as seen in conditions like keratitis or dystrophy.[1]
Anatomy
Gross Anatomy
The cornea is the transparent, dome-shaped anterior portion of the eye's outer fibrous tunic, forming a convex continuation of the opaque sclera and covering the iris and pupil to allow light entry into the anterior chamber.[8] Positioned at the front of the globe, it occupies roughly the anterior one-sixth of the ocular surface, providing structural integrity and the primary refractive interface for vision.[1]In adults, the cornea exhibits a horizontally oval shape, with a horizontal diameter of approximately 11–12 mm and a vertical diameter of 9–11 mm.[9] Its thickness varies regionally, measuring about 0.5–0.6 mm at the center and increasing to 0.6–0.8 mm peripherally due to the thickening of its stromal layer.[10] The anterior surface has a radius of curvature of roughly 7.8 mm, while the posterior surface is steeper with a radius of about 6.8 mm, resulting in a prolate aspheric form that enhances optical performance.[11] This geometry accounts for approximately 40–44 diopters of the eye's total refractive power, comprising two-thirds of the overall focusing capability.[2]The cornea interfaces with adjacent structures at its periphery, where it junctions with the sclera at the limbus—a narrow transitional zone approximately 1 mm wide that demarcates the corneal and scleral boundaries.[12] The overlying conjunctiva, which covers the sclera, merges with the corneal surface at the limbus, facilitating a smooth epithelial transition.[12] Anteriorly, the cornea is coated by the precorneal tear film, a thin multilayered fluid that maintains hydration, provides refractive smoothness, and protects against environmental insults.[2]
Layers and Microstructure
The human cornea consists of five primary histological layers, each contributing to its overall microstructure and transparency: the epithelium, Bowman's layer, stroma, Descemet's membrane, and endothelium.[1] These layers are arranged from anterior to posterior, with the cornea being notably avascular throughout, relying on diffusion from the tear film and aqueous humor for nutrient supply.[13]The outermost layer, the corneal epithelium, is a stratified squamous non-keratinized epithelium approximately 50 μm thick, comprising 5–6 layers of cells divided into superficial (2–3 layers), wing (2–3 layers), and basal cells.[2] Basal cells are cuboidal and mitotically active, anchored to the underlying basement membrane via hemidesmosomes, while superficial cells are flattened and connected by tight junctions to provide a barrier; the epithelium is regenerative, with stem cells located at the limbal region.[14]Beneath the epithelium lies Bowman's layer, an acellular, condensed layer of randomly oriented type I and III collagen fibrils, measuring 8–12 μm in thickness.[13] This layer serves as a protective interface, transitioning abruptly from the epithelial basement membrane to the more organized stromal collagen.[1]The stroma constitutes about 90% of the corneal thickness (approximately 450–500 μm), forming the bulk of the tissue with an avascular matrix populated by sparse keratocytes (fibroblast-like cells) embedded in a highly organized extracellular matrix.[15] Its transparency arises from parallel lamellae of uniformly thin, orthogonal type I collagen fibrils arranged in approximately 200–300 stacked layers, with minimal extracellular proteoglycans maintaining uniform interfibrillar spacing.[13]Some anatomical models recognize an additional layer, Dua's layer (also known as the pre-Descemet's layer), a distinct acellular band of 10–15 μm thickness located at the posterior limit of the stroma. Composed of 5–8 tightly packed lamellae of type I collagen with minimal elastin, it provides significant tensile strength to the cornea and is impervious to air.[16]Descemet's membrane is the elastic basement membrane secreted by the endothelium, initially 3–4 μm thick in youth but thickening progressively with age to 10–12 μm or more due to banded collagen deposition.[1] It consists of an anterior non-banded zone and a posterior banded zone with hexagonal lattice-like collagen fibers.[2]The innermost endothelium is a single monolayer of flattened, polygonal (typically hexagonal) cells, about 4–5 μm thick, with limited regenerative capacity in adults.[4] These cells feature tight junctions and contain numerous mitochondria, reflecting their role in maintaining corneal hydration through active transport mechanisms.[1]
Innervation and Vascular Supply
The cornea receives its sensory innervation primarily from the long ciliary nerves, which are branches of the ophthalmic division of the trigeminal nerve (cranial nerve V1).[17] These nerves enter the corneal stroma from the periphery and branch extensively to form a dense sub-basal nerve plexus beneath the basal epithelium, from which free nerve endings extend into the epithelium.[18] These sensory endings detect mechanical, thermal, and chemical stimuli, mediating protective reflexes such as blinking and lacrimal gland stimulation for tear production.[17]The corneal epithelium exhibits the highest nerve density of any human tissue, with approximately 7,000 free nerve endings per square millimeter.[19] This extraordinary innervation density, which is 300 to 600 times greater than that of the skin, underscores the cornea's acute sensitivity to protect its surface integrity.[19]The cornea is completely avascular, lacking blood vessels throughout its structure to preserve optical transparency by minimizing light scattering from vascular elements.[2] Nutrients such as glucose and amino acids diffuse primarily from the aqueous humor anteriorly through the stroma, while oxygen is obtained mainly from the tear film and atmospheric exposure; additional solutes reach the peripheral cornea via perilimbal capillaries.[20]Lymphatic drainage is absent in the cornea, consistent with its avascular nature.[21] Immune surveillance is instead maintained by resident antigen-presenting cells, including Langerhans cells in the epithelium, which detect and respond to pathogens without relying on lymphatic transport.[22]
Development and Physiology
Embryonic Development
The development of the cornea originates from interactions between the surface ectoderm and neural crest-derived mesenchyme during early human embryogenesis. At approximately the fourth week of gestation, the optic vesicle induces the overlying surface ectoderm to form the lens placode, marking the initiation of lens and corneal development.[23] By the fifth week, the lens placode invaginates and detaches to form the lens vesicle, while the surface ectoderm differentiates into the corneal epithelium, a multilayered structure that initially remains in close apposition to the lens.[2] Neural crest cells then migrate in successive waves into the periocular region: the first wave occupies the space between the lens vesicle and epithelium to initiate stromal formation, the second wave contributes to the endothelial layer, and the third wave supports iris and trabecular meshwork development.[24]Key developmental events follow this foundational stage. Around the third month of gestation (approximately week 12), the hyaloid artery—which provides transient vascular supply to the lens and retina—begins to regress as the retinal vasculature emerges, ensuring the cornea's eventual avascularity.[25] By the 20th gestational week, the cornea attains transparency, driven by the organized deposition of extracellular matrix in the stroma and the establishment of regular collagen fibril spacing that minimizes light scattering.[26] This transparency is essential for fetal visual development and coincides with eyelid fusion, which protects the maturing ocular surface until birth.[27]Postnatal maturation refines the corneal structure. The endothelial cell density starts high at birth, approximately 5,000 cells/mm², and progressively decreases to adult levels of around 2,500 cells/mm² due to limited proliferative capacity and natural attrition.[28]Bowman's layer, an acellular condensation of collagen beneath the epithelium, forms postnatally from processes of superficial stromal keratocytes, typically completing around 6 months of age and contributing to epithelial-stromal adhesion.[29]Defects in neural crest migration can lead to congenital anomalies like Peters anomaly, characterized by central corneal opacification, iridocorneal adhesions, and lens-cornea synechiae due to failed separation of the lens vesicle from the endothelium.[24]
Optical Physiology
The cornea serves as the primary refractive element of the eye, contributing approximately two-thirds of its total optical power, equivalent to about 43 diopters.[30] This high refractive power arises from the cornea's anterior curvature and its refractive index of 1.376, which contrasts sharply with the surrounding air (index 1.000) and aqueous humor (index 1.336).[30] Unlike the crystalline lens, the cornea maintains a fixed curvature and does not undergo active changes during accommodation; instead, it provides a stable refractive base that works in tandem with the lens to focus light onto the retina.[31]The cornea's optical efficacy stems from its transparency and precise lightrefraction, enabled by the organized arrangement of collagenfibrils in the stroma, which creates a graded refractive index across the tissue.[32] According to lattice theory, the uniform diameter and regular spacing of these fibrils—typically 25–35 nm in diameter with inter-fibril distances of about 55–60 nm—minimize lightscattering by ensuring destructive interference of scattered waves, thus preserving clarity.[33] This structural regularity is complemented by deturgescence, where the endothelial layer actively pumps ions to maintain stromal hydration at approximately 78% water content, preventing swelling that could disrupt fibril organization and induce opacity.[30]Additionally, the cornea's prolate aspheric shape, characterized by a negative asphericity (Q value around -0.26), inherently corrects for spherical aberration, producing minimal positive spherical aberration compared to a spherical surface.[34] This geometric feature balances the positive spherical aberration from the lens, optimizing overall image quality on the retina without additional muscular adjustments.[34]
Protective and Metabolic Functions
The corneal epithelium serves as the primary physical barrier against environmental threats, with its superficial layer forming tight junctions that prevent the ingress of pathogens, allergens, and mechanical trauma into deeper tissues.[35] These junctions, composed of proteins such as claudins and occludins, create a selective permeability seal that maintains the integrity of the underlying stroma while allowing nutrient diffusion.[36] Complementing this, the tear film's mucin layer, primarily secreted by conjunctival goblet cells, enhances adhesion to the epithelial glycocalyx, providing lubrication and trapping particulates to reduce shear forces and microbial attachment during blinking.[37]In response to injury, the cornea exhibits robust wound healing mechanisms to restore barrier function swiftly. Epithelial defects heal rapidly through proliferation and migration of cells derived from limbal stem cells located at the corneoscleral junction, enabling coverage of small wounds within hours to days and preventing secondary infections.[38] Deeper stromal injuries trigger keratocytes—quiescent stromal fibroblasts—to activate into myofibroblasts, which deposit extracellular matrix for remodeling, though excessive fibrosis can temporarily compromise transparency until resolution.[39]Due to its avascular nature, the cornea relies predominantly on anaerobic glycolysis for energy production, with approximately 85% of glucose metabolism occurring via this pathway in epithelial and endothelial cells to generate ATP under low-oxygen conditions.[40] The endothelium maintains stromal dehydration through active transport via Na+/K+-ATPase pumps, which expel fluid at a rate of 10-15 μl/cm²/hour, countering passive leakage from the aqueous humor to preserve corneal thickness and clarity.[41]The cornea balances immune surveillance with minimal inflammation to safeguard transparency. Resident antigen-presenting cells, such as dendritic cells in the epithelium and stroma, detect and process pathogens but promote immune privilege by inducing regulatory T cells rather than robust effector responses, thereby limiting vascularization and opacity-inducing inflammation.[42] A unique protective mechanism involves the blink reflex, mediated by trigeminal nerve afferents, which mechanically clears debris and distributes tears for lubrication approximately 15-20 times per minute under normal conditions.[17]
Disorders and Clinical Significance
Common Disorders
Keratitis represents one of the most prevalent corneal disorders, characterized by inflammation of the corneal tissue that can lead to significant visual impairment if severe. Infectious keratitis is primarily caused by bacterial pathogens such as Pseudomonas aeruginosa in contact lens wearers, viral agents like herpes simplex virus (HSV), or fungal organisms, often entering through epithelial defects from trauma or poor hygiene. Symptoms typically include acute eye pain, photophobia, redness, tearing, and blurred vision due to corneal edema and infiltrates. [43][44][45]Sterile, or non-infectious, keratitis arises from mechanical irritation, such as prolonged exposure from incomplete eyelid closure or overwear of contact lenses, leading to epithelial breakdown without microbial invasion. These cases present with similar symptoms of pain, photophobia, and foreign body sensation, though less likely to form ulcers. Emerging research highlights the potential role of the ocular surface microbiome in predisposing to non-infectious keratitis, where dysbiosis may exacerbate inflammation in conditions like dry eye syndrome by altering immune homeostasis on the cornea. [43][46]Keratoconus is a progressive ectatic disorder involving corneal thinning and bulging into a cone-like shape, typically onsetting in adolescence or early adulthood. Its etiology involves a combination of genetic and environmental factors, including chronic eye rubbing and atopy. Candidate genes such as VSX1 and SOD1 have been investigated, but their causative role remains unconfirmed across studies. This leads to irregular astigmatism, distorted vision, and increased light sensitivity as the corneal curvature steepens asymmetrically. [47][48][49]Corneal dystrophies encompass a group of hereditary conditions affecting specific corneal layers, with Fuchs' endothelial dystrophy being the most common in older adults, characterized by progressive endothelial cell failure and formation of guttae (excrescences) on the Descemet membrane. Lattice dystrophy, another stromal variant, results from amyloid protein deposits forming branching, glass-like lines in the corneal stroma. Both manifest with symptoms of blurred or hazy vision, glare, and recurrent epithelial erosions, worsening over time due to stromal haze and edema. [50][51]Dry eye syndrome exerts a notable impact on the cornea through diminished tear film stability and inadequate lubrication, which can cause superficial punctate erosions and compromise the epithelial barrier. Reduced tear production or rapid evaporation leads to increased friction during blinking, resulting in corneal surface damage, stinging sensations, scratchiness, and fluctuating blurry vision. [52][53]Corneal trauma, including abrasions and chemical burns, constitutes a major category of acute disorders, where mechanical scratches from foreign bodies disrupt the epithelium, causing immediate pain, tearing, and light sensitivity. Chemical burns vary in severity; acid injuries cause superficial coagulationnecrosis, while alkali burns penetrate deeper due to saponification of cell membranes and proteins, leading to liquefactive necrosis, limbal stem cell loss, and prolonged inflammation. [54][55]
Diagnostic Approaches
Diagnostic approaches to assessing corneal health, structure, and function rely on a combination of clinical examinations and advanced imaging techniques to evaluate transparency, thickness, curvature, cellular integrity, and surface integrity. These methods enable early detection of abnormalities such as opacities, thinning, ectasias, endothelial dysfunction, and epithelial defects, which are critical for timely intervention. Slit-lamp biomicroscopy serves as the cornerstone of corneal evaluation, providing magnified visualization of the corneal layers, detection of opacities, and assessment of the endothelium through specular reflection from the posterior surface.[56][57][58] By adjusting the slit beam's angle and width, clinicians can identify subtle changes in stromal clarity or endothelial guttae, often enhanced by specular microscopy integration for detailed reflection analysis.[59][60]Pachymetry measures corneal thickness, essential for assessing edema or thinning, with the normal central corneal thickness averaging approximately 540 μm in healthy adults.[61] This can be performed using ultrasound pachymetry, which provides contact-based measurements, or non-contact optical coherence tomography (OCT), offering high-resolution data without anesthesia.[62] Variations in thickness, such as increased values in edema or decreased in ectasias, guide risk stratification for conditions like glaucoma or refractive surgery.[63]Corneal topography and keratometry map the corneal curvature to detect irregularities, particularly ectasias like keratoconus, by analyzing anterior surface elevation and power.[64] Placido disc-based systems project concentric rings onto the cornea to assess mires for asymmetry, while Scheimpflug imaging provides tomographic data on both anterior and posterior surfaces, improving ectasia detection through posterior elevation maps.[65][66] These techniques quantify steepening or thinning, with indices like the inferior-superior value aiding in early diagnosis.[67]In vivo confocal microscopy enables non-invasive, high-resolution imaging of corneal cellular structures, particularly the endothelium, where cell density below 2,000 cells/mm² signals increased risk of decompensation.[68] This laser scanning method visualizes hexagonal endothelial cells, pleomorphism, and polymegathism, correlating well with specular microscopy for quantitative analysis in diseased states.[69][70]Vital staining assesses epithelial integrity by highlighting defects and devitalized tissue. Fluorescein dye, applied topically, pools in epithelial erosions or ulcers under cobalt blue illumination, delineating surface breaks.[71]Rose bengal, a fluorescein derivative, stains devitalized or mucin-deficient cells pink, offering superior detection of subtle ocular surface damage compared to fluorescein alone.[72][73]Anterior segment OCT provides detailed cross-sectional views of the cornea, surpassing traditional methods by quantifying layer-specific thickness, opacities, and stromal details with micrometer resolution.[74] This non-contact imaging modality visualizes the full corneal depth, including the endothelium and Descemet's membrane, facilitating precise evaluation of pathologies like dystrophies or post-surgical changes.[75][76]
Treatment Options
Treatment of corneal conditions often begins with non-surgical approaches aimed at addressing infection, inflammation, epithelial integrity, and structural stability. Pharmacological interventions are a cornerstone, particularly for infectious keratitis. For bacterial keratitis, topical fluoroquinolone antibiotics such as gatifloxacin 0.3% are commonly prescribed due to their broad-spectrum activity against gram-positive and gram-negative pathogens, demonstrating comparable efficacy to fortified antibiotics in clinical trials while offering the convenience of monotherapy.[77] Viral keratitis, such as herpes simplex virus epithelial keratitis, is managed with topical antivirals like ganciclovir 0.15% gel or trifluridine 1% solution, which exhibit similar effectiveness in resolving dendritic lesions and promoting epithelial healing.[78] Topical corticosteroids, such as prednisolone acetate, may be used adjunctively to control inflammation in non-infectious or post-infectious scenarios, but their application requires caution due to the risk of potentiating corneal melting through inhibition of collagen synthesis and increased ulceration potential, particularly in active infections.[79]For dry eye syndrome, which can compromise the corneal surface and lead to epitheliopathy, artificial tear lubricants provide symptomatic relief by supplementing the tear film and reducing evaporation, while punctal plugs occlude the lacrimal drainage points to retain natural tears and enhance ocular surface wetting.[80] These conservative measures have been shown to alleviate symptoms, stabilize the tear film, and repair superficial corneal lesions in moderate cases.[81] In instances of persistent epithelial defects, such as those from trauma or neurotrophic keratitis, therapeutic bandage contact lenses facilitate healing by protecting the denuded stroma, promoting epithelial migration, and alleviating pain, often outperforming traditional patching in accelerating re-epithelialization.[82]Specialty contact lenses offer vision rehabilitation for structural irregularities without invasive intervention. In keratoconus, where progressive thinning causes irregular astigmatism, scleral lenses vault over the cornea to create a smooth refractive surface with a fluid reservoir, improving visual acuity and comfort for patients intolerant to standard lenses.[83]Orthokeratology lenses, worn overnight, temporarily reshape the corneal epithelium to correct mild irregular astigmatism, providing spectacle-free daytime vision and potentially slowing progression in early disease.[84]Corneal collagen cross-linking (CXL) serves as a non-surgical adjunct to stabilize progressive ectatic disorders like keratoconus by inducing stromal stiffening through riboflavin (vitamin B2) sensitization followed by ultraviolet-A (UVA) irradiation at 365 nm, a method expanded in FDA approval in 2016 for epithelium-off application in patients aged 14 and older. In October 2025, the FDA approved Epioxa (riboflavin 5'-phosphate ophthalmic solution) for epithelium-on CXL to treat keratoconus in patients aged 13 and older, offering a non-invasive alternative without epithelial removal.[85] This photochemical process increases corneal biomechanical strength by up to 300% without altering the anterior curvature significantly, halting ectasia in over 90% of treated eyes based on long-term follow-up studies.[86][87]Nutritional deficiencies contributing to corneal pathology, such as vitamin A deficiency leading to xerophthalmia and keratomalacia, are addressed through oral supplementation with high-dose retinol (e.g., 200,000 IU for children over 12 months), which reverses night blindness and corneal xerosis within weeks when initiated early.[88] Emerging biologic therapies, including amniotic membrane extracts in eye drop formulations, provide anti-inflammatory benefits by modulating cytokine expression and promoting epithelial repair in inflammatory corneal conditions refractory to standard treatments.[89] If non-surgical options fail to control progression, escalation to surgical interventions may be necessary.
Surgical Interventions and Transplantation
Surgical interventions for corneal disorders primarily involve procedures aimed at repairing or replacing damaged tissue to restore optical clarity and function. Phototherapeutic keratectomy (PTK) utilizes an excimer laser to ablate superficial corneal opacities and irregularities, effectively treating conditions such as corneal dystrophies, recurrent erosions, and band keratopathy by removing micrometers of tissue with high precision while preserving deeper layers.[90][91] For stromal pathologies not involving the endothelium, deep anterior lamellar keratoplasty (DALK) replaces the anterior cornea down to Descemet's membrane, minimizing rejection risk by retaining the recipient's healthy endothelium and offering improved tectonic stability compared to full-thickness procedures.[92][93]Corneal transplantation, or keratoplasty, encompasses full-thickness and partial-thickness techniques tailored to the affected layer. Penetrating keratoplasty (PK) involves excising and replacing the entire corneal thickness, commonly used for advanced keratoconus, scars, or perforations, with clear graft success rates exceeding 90% in the first year postoperatively.[94]Endothelial keratoplasty, including Descemet stripping endothelial keratoplasty (DSEK) and Descemet stripping automated endothelial keratoplasty (DSAEK), targets Fuchs' endothelial dystrophy by replacing only the dysfunctional endothelium and Descemet's membrane with a thin donor stromal layer, achieving rapid visual rehabilitation and lower suture-related complications.[95][96]Donor corneas are sourced from accredited eye banks, where tissue is rigorously screened for viability and infectious risks before preservation in media like Optisol-GS, allowing storage for up to 14 days at 2-6°C to maintain endothelial cell density.[97]Human leukocyte antigen (HLA) matching is not routinely performed for most corneal transplants due to the cornea's immune privilege, though it may be considered in high-risk cases.[98]Postoperative complications include graft rejection, most frequently affecting the endothelium in PK and endothelial keratoplasties, as well as astigmatism from irregular wound healing or suture tension.[99] Standard management involves topical corticosteroids to suppress inflammation and prevent rejection, tapered over months based on clinical response.[100]Recent advances enhance precision and accessibility in these procedures. Femtosecond laser-assisted PK, adopted widely since the 2010s, enables customized, zigzag incisions for better wound apposition, reducing astigmatism and accelerating recovery.[101] Bioengineered corneas, such as hydrogel-based implants, are in clinical trials; as of 2025, ongoing clinical trials and pre-clinical advancements, such as positive FDA meetings in February 2025 and collaborations like Pantheon Vision with Eyedeal Medical in March 2025, demonstrate promising progress in bioengineered corneal implants for integration and transparency restoration in patients with stromal defects, potentially alleviating donor shortages.[102][103][104][105] Global corneal tissue shortages persist, affecting millions in developing regions, but initiatives like those from the Lions World Vision Institute facilitate international distribution and training to increase supply and equity.[106][107]