Recent from talks
Pyomyositis
Knowledge base stats:
Talk channels stats:
Members stats:
Pyomyositis
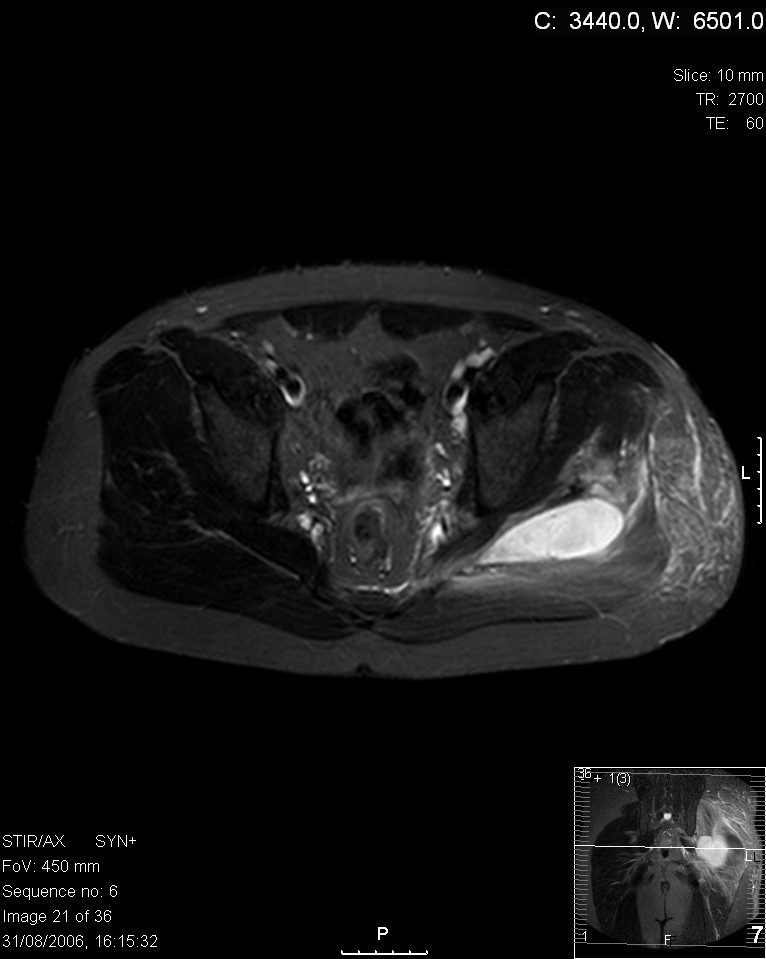
Pyomyositis (Myositis tropicans) is a bacterial infection of the skeletal muscles which results in an abscess. Pyomyositis is most common in tropical areas but can also occur in temperate zones.
Pyomyositis can be classified as primary or secondary. Primary pyomyositis is a skeletal muscle infection arising from hematogenous infection, whereas secondary pyomyositis arises from localized penetrating trauma or contiguous spread to the muscle.
Diagnosis is done via the following manner:
Bioptates of affected muscle tissues show acute and chronic inflammatory cells, and in one case caused by influenza A infection muscle cells show lack of nuclei.
Pyogenic symptoms usually are present in the following muscles:
The course of this disease is divided into three distinct phases. The invasive stage manifests as general muscle soreness and swelling without erythema and low-grade fever and lasts about ten days. The purulent-suppurative stage occurs after about 2–3 weeks and is associated with increased body temperature and muscle tenderness. In the third stage, sepsis occurs that can lead to serious complications, including death.
The abscesses within the muscle must be drained surgically (not all patients require surgery if there is no abscess). Antibiotics, such as vancomycin, teicoplanin, tigecycline, daptomycin or linezolid are given for a minimum of three weeks to clear the infection. In some cases, co-trimoxazole is sufficient.
Pyomyositis is most often caused by the bacterium Staphylococcus aureus. The infection can affect any skeletal muscle, but most often infects the large muscle groups such as the quadriceps or gluteal muscles.
Hub AI
Pyomyositis AI simulator
(@Pyomyositis_simulator)
Pyomyositis
Pyomyositis (Myositis tropicans) is a bacterial infection of the skeletal muscles which results in an abscess. Pyomyositis is most common in tropical areas but can also occur in temperate zones.
Pyomyositis can be classified as primary or secondary. Primary pyomyositis is a skeletal muscle infection arising from hematogenous infection, whereas secondary pyomyositis arises from localized penetrating trauma or contiguous spread to the muscle.
Diagnosis is done via the following manner:
Bioptates of affected muscle tissues show acute and chronic inflammatory cells, and in one case caused by influenza A infection muscle cells show lack of nuclei.
Pyogenic symptoms usually are present in the following muscles:
The course of this disease is divided into three distinct phases. The invasive stage manifests as general muscle soreness and swelling without erythema and low-grade fever and lasts about ten days. The purulent-suppurative stage occurs after about 2–3 weeks and is associated with increased body temperature and muscle tenderness. In the third stage, sepsis occurs that can lead to serious complications, including death.
The abscesses within the muscle must be drained surgically (not all patients require surgery if there is no abscess). Antibiotics, such as vancomycin, teicoplanin, tigecycline, daptomycin or linezolid are given for a minimum of three weeks to clear the infection. In some cases, co-trimoxazole is sufficient.
Pyomyositis is most often caused by the bacterium Staphylococcus aureus. The infection can affect any skeletal muscle, but most often infects the large muscle groups such as the quadriceps or gluteal muscles.
Recent media