

Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Cleft lip and cleft palate
View on Wikipedia
| Cleft lip and palate | |
|---|---|
| Other names | Hare-lip, cleft lip and palate |
 | |
| Child with cleft lip and palate | |
| Specialty | Oral and Maxillofacial Surgery, Otorhinolaryngology, pediatrics |
| Symptoms | Opening in the upper lip that may extend into the nose or palate[1] |
| Complications | Feeding problems, speech problems, hearing problems, frequent ear infections[1] |
| Usual onset | Present at birth[1] |
| Causes | Usually unknown[1] |
| Risk factors | Smoking during pregnancy, diabetes, obesity, older mother, certain medications[1][2] |
| Treatment | Surgery, speech therapy, dental care[1] |
| Prognosis | Good (with treatment)[1] |
| Frequency | 1.5 per 1000 births (developed world)[2] |
| Deaths | 3,800 (2017)[3] |
A cleft lip contains an opening in the upper lip that may extend into the nose.[1] The opening may be on one side, both sides, or in the middle.[1] A cleft palate occurs when the palate (the roof of the mouth) contains an opening into the nose.[1] The term orofacial cleft refers to either condition or to both occurring together. These disorders can result in feeding problems, speech problems, hearing problems, and frequent ear infections.[1] Less than half the time the condition is associated with other disorders.[1]
Cleft lip and palate are the result of tissues of the face not joining properly during development.[1] As such, they are a type of birth defect.[1] The cause is unknown in most cases.[1] Risk factors include smoking during pregnancy, diabetes, obesity, an older mother, and certain medications (such as some used to treat seizures).[1][2] Cleft lip and cleft palate can often be diagnosed during pregnancy with an ultrasound exam.[1]
A cleft lip or palate can be successfully treated with surgery.[1] This is often done in the first few months of life for cleft lip and before eighteen months for cleft palate.[1] Speech therapy and dental care may also be needed.[1] With appropriate treatment, outcomes are good.[1]
Cleft lip and palate occurs in about 1 to 2 per 1000 births in the developed world.[2] Cleft lip is about twice as common in males as females, while cleft palate without cleft lip is more common in females.[2] In 2017, it resulted in about 3,800 deaths globally, down from 14,600 deaths in 1990.[3][4] Cleft lips are commonly known as hare-lips because of their resemblance to the lips of hares or rabbits, although that term is considered to be offensive in certain contexts.[5]
Signs and symptoms
[edit]Cleft lip
[edit]If the cleft does not affect the palate structure of the mouth, it is referred to as cleft lip. Cleft lip is formed in the top of the lip as either a small gap or an indentation in the lip (partial or incomplete cleft), or it continues into the nose (complete cleft). Lip cleft can occur as a one-sided (unilateral) or two-sided (bilateral) condition. It is due to the failure of fusion of the maxillary prominence and medial nasal processes (formation of the primary palate).
-
 Unilateral incomplete
Unilateral incomplete -
 Unilateral complete
Unilateral complete -
 Bilateral complete
Bilateral complete



A mild form of a cleft lip is a microform cleft.[6] A microform cleft can appear as small as a little dent in the red part of the lip or look like a scar from the lip up to the nostril.[7] In some cases muscle tissue in the lip underneath the scar is affected and might require reconstructive surgery.[8] It is advised to have newborn infants with a microform cleft checked with a craniofacial team as soon as possible to determine the severity of the cleft.[9]
-
 Six-month-old girl before going into surgery to have her unilateral complete cleft lip repaired
Six-month-old girl before going into surgery to have her unilateral complete cleft lip repaired -
 The same girl, one month after the surgery
The same girl, one month after the surgery -
 The same girl, age eight, the scar almost gone
The same girl, age eight, the scar almost gone



Cleft palate
[edit]Cleft palate is a condition in which the two plates of the skull that form the hard palate (roof of the mouth) are not completely joined. The soft palate is in these cases cleft as well. In most cases, cleft lip is also present.
Palate cleft can occur as complete (soft and hard palate, possibly including a gap in the jaw) or incomplete (a 'hole' in the roof of the mouth, usually as a cleft soft palate). When cleft palate occurs, the uvula is usually split. It occurs due to the failure of fusion of the lateral palatine processes, the nasal septum, or the median palatine processes (formation of the secondary palate).
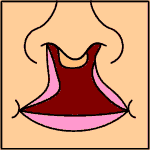
The hole in the roof of the mouth caused by a cleft connects the mouth directly to the inside of the nose.
Note: the next images show the roof of the mouth. The top shows the nose, the lips are colored pink. For clarity the images depict a toothless infant.
-
 Incomplete cleft palate
Incomplete cleft palate -
 Unilateral complete lip and palate
Unilateral complete lip and palate -
 Bilateral complete lip and palate
Bilateral complete lip and palate



A result of an open connection between the mouth and inside the nose is called velopharyngeal insufficiency (VPI). Because of the gap, air leaks into the nasal cavity resulting in a hypernasal voice resonance and nasal emissions while talking.[10] Secondary effects of VPI include speech articulation errors (e.g., distortions, substitutions, and omissions) and compensatory misarticulations and mispronunciations (e.g., glottal stops and posterior nasal fricatives).[11] Possible treatment options include speech therapy, prosthetics, augmentation of the posterior pharyngeal wall, lengthening of the palate, and surgical procedures.[10]
Submucous cleft palate can also occur, which is a cleft of the soft palate with a split uvula, a furrow along the midline of the soft palate, and a notch in the back margin of the hard palate.[12] The diagnosis of submucous cleft palate often occurs late in children as a result of the nature of the cleft.[13] While the muscles of the soft palate are not joined, the mucosal membranes covering the roof of the mouth appear relatively normal and intact.[14]
Teeth
[edit]Tooth development can be delayed with increasing severity of CLP. Some of the dental problems affect the primary teeth, but most of the problems arise after the permanent teeth erupt. Problems may include fused teeth, missing teeth, and extra teeth erupting behind normal teeth. Missing teeth or extra teeth are both normal occurrences. Typically, the lateral incisors are missing. The enamel (outermost layer of the tooth) is commonly found to be hypomineralized and hypoplastic, making the teeth more likely to decay. As CLP can make oral hygiene more difficult, there is an increased rate of cavities.[15] In addition, abnormal positioning of individual teeth may affect occlusion, which can create an open bite or cross bite. This in turn can then affect the patient's speech.[16][17]
Complications
[edit]
Cleft may cause problems with feeding, ear disease, speech, socialization, and cognition.
Due to lack of suction, an infant with a cleft may have trouble feeding. An infant with a cleft palate will have greater success feeding in a more upright position, as gravity will help prevent milk from coming through the baby's nose. Gravity feeding can be accomplished by using specialized equipment, such as the Haberman Feeder. Another equipment commonly used for gravity feeding is a customized bottle with a combination of nipples and bottle inserts. A large hole, crosscut, or slit in the nipple, a protruding nipple and rhythmically squeezing the bottle insert can result in controllable flow to the infant without the stigma caused by specialized equipment.
Individuals with cleft also face many middle ear infections which may eventually lead to hearing loss. The Eustachian tubes and external ear canals may be angled or tortuous, leading to food or other contamination of a part of the body that is normally self-cleaning. Hearing is related to learning to speak. Babies with palatal clefts may have compromised hearing and therefore, if the baby cannot hear, it cannot try to mimic the sounds of speech. Thus, even before expressive language acquisition, the baby with the cleft palate is at risk for receptive language acquisition. Because the lips and palate are both used in pronunciation, individuals with cleft usually need the aid of a speech therapist.
Tentative evidence has found that those with clefts perform less well at language.[18]
Psychosocial issues
[edit]There is research dedicated to the psychosocial development of individuals with cleft palate. A cleft palate/lip may impact an individual's self-esteem, social skills and behavior. Self-concept may be adversely affected by the presence of a cleft lip or cleft palate, particularly among girls.[19] Negative outcomes can also be associated with the long durations of hospitalization. Psychological issues could extend not just to the individual with CLP but also to their families, particularly their mothers, that experience varying levels of depression and anxiety.[20][21]
Research has shown that during the early preschool years (ages 3–5), children with cleft lip or cleft palate tend to have a self-concept that is similar to their peers without a cleft. However, as they grow older and their social interactions increase, children with clefts tend to report more dissatisfaction with peer relationships and higher levels of social anxiety. Experts conclude that this is probably due to the associated stigma of visible deformities and possible speech impediments. Children who are judged as attractive tend to be perceived as more intelligent, exhibit more positive social behaviors, and are treated more positively than children with cleft lip or cleft palate.[22] Children with clefts tend to report feelings of anger, sadness, fear, and alienation from their peers, but these children were similar to their peers in regard to "how well they liked themselves."
The relationship between parental attitudes and a child's self-concept is crucial during the preschool years. It has been reported that elevated stress levels in mothers correlated with reduced social skills in their children.[23] Strong parent support networks may help to prevent the development of negative self-concept in children with cleft palate.[24] In the later preschool and early elementary years, the development of social skills is no longer only impacted by parental attitudes but is beginning to be shaped by their peers. A cleft lip or cleft palate may affect the behavior of preschoolers. Experts suggest that parents discuss with their children ways to handle negative social situations related to their cleft lip or cleft palate. A child who is entering school should learn the proper (and age-appropriate) terms related to the cleft. The ability to confidently explain the condition to others may limit feelings of awkwardness and embarrassment and reduce negative social experiences.[25]
As children reach adolescence, the period of time between age 13 and 19, the dynamics of the parent-child relationship change as peer groups are now the focus of attention. An adolescent with cleft lip or cleft palate will deal with the typical challenges faced by most of their peers including issues related to self-esteem, dating and social acceptance.[26][27][28] Adolescents, however, view appearance as the most important characteristic, above intelligence and humor.[29] This being the case, adolescents are susceptible to additional problems because they cannot hide their facial differences from their peers. Adolescent boys typically deal with issues relating to withdrawal, attention, thought, and internalizing problems, and may possibly develop anxiousness-depression and aggressive behaviors.[28] Adolescent girls are more likely to develop problems relating to self-concept and appearance. Individuals with cleft lip or cleft palate often deal with threats to their quality of life for multiple reasons including unsuccessful social relationships, deviance in social appearance, and multiple surgeries.
Cause
[edit]Most clefts are polygenic and multifactorial in origin with many genetic and environmental factors contributing. Genetic factors cause clefts in 20% to 50% of the cases and the remaining clefts are attributable to either environmental factors (such as teratogens) or gene-environment interactions. The polygenic/multifactorial inheritance model predicts that most individuals will be born without clefts; however with a number of genetic or environmental factors, it can result in cleft formation.[17]
The development of the face is coordinated by complex morphogenetic events and rapid proliferative expansion, and is thus highly susceptible to environmental and genetic factors, rationalising the high incidence of facial malformations. During the first six to eight weeks of pregnancy, the shape of the embryo's head is formed. Five primitive tissue lobes grow:
- a) one from the top of the head down towards the future upper lip (frontonasal prominence);
- b-c) two from the cheeks, which meet the first lobe to form the upper lip (maxillar prominence);
- d-e) and just below, two additional lobes grow from each side, which form the chin and lower lip (mandibular prominence).
If these tissues fail to meet, a gap appears where the tissues should have joined (fused). This may happen in any single joining site, or simultaneously in several or all of them. The resulting birth defect reflects the locations and severity of individual fusion failures (e.g., from a small lip or palate fissure up to a completely malformed face).
The upper lip is formed earlier than the palate, from the first three lobes named a to c above. Formation of the palate is the last step in joining the five embryonic facial lobes, and involves the back portions of the lobes b and c. These back portions are called palatal shelves, which grow towards each other until they fuse in the middle.[30] This process is very vulnerable to multiple toxic substances, environmental pollutants, and nutritional imbalance. The biologic mechanisms of mutual recognition of the two cabinets, and the way they are glued together, are quite complex and obscure despite intensive scientific research.[30]
Orofacial clefts may be associated with a syndrome (syndromic) or may not be associated with a syndrome (nonsyndromic). Syndromic clefts are part of syndromes that are caused by a variety of factors such as environment and genetics or an unknown cause. Nonsyndromic clefts, which are not as common as syndromic clefts, also have a genetic cause.[31]
Genetics
[edit]Genetic factors contributing to cleft lip and cleft palate formation have been identified for some syndromic cases. Many clefts run in families, even though in some cases there does not seem to be an identifiable syndrome present.[32] A number of genes are involved including cleft lip and palate transmembrane protein 1 and GAD1,[33] One study found an association between mutations in the HYAL2 gene and cleft lip and cleft palate formation.[34]
Syndromes
[edit]- The Van der Woude syndrome is caused by a specific variation in the gene IRF6 that increases the occurrence of these deformities threefold.[35][36][37] Mutations in interferon regulatory factor 6 (IRF6) that cause cleft lip palate are also implicated in neural tube defects such as spina bifida.[38]
- Another syndrome, Siderius X-linked intellectual disability, is caused by mutations in the PHF8 gene (OMIM: 300263); in addition to cleft lip or palate, symptoms include facial dysmorphism and mild intellectual disability.[39]
In some cases, cleft palate is caused by syndromes that also cause other problems:
- Stickler syndrome can cause cleft lip and palate, joint pain, and myopia.[40][41]
- Loeys–Dietz syndrome can cause cleft palate or bifid uvula, hypertelorism, and aortic aneurysm.[42]
- Hardikar syndrome can cause cleft lip and palate, Hydronephrosis, Intestinal obstruction and other symptoms.[43]
- Cleft lip/palate may be present in many different chromosome disorders including Patau syndrome (trisomy 13).
- Malpuech facial clefting syndrome
- Hearing loss with craniofacial syndromes
- Popliteal pterygium syndrome
- Cornelia de Lange syndrome
- Treacher Collins syndrome
- Pierre Robin syndrome[44][31]
Specific genes
[edit]| Type | OMIM | Gene | Locus |
|---|---|---|---|
| OFC1 | 119530 | ? | 6p24 |
| OFC2 | 602966 | ? | 2p13 |
| OFC3 | 600757 | ? | 19q13 |
| OFC4 | 608371 | ? | 4q |
| OFC5 | 608874 | MSX1 | 4p16.1 |
| OFC6 | 608864 | ? | 1q |
| OFC7 | 600644) | PVRL1 | 11q |
| OFC8 | 129400 | TP63 | 3q27 |
| OFC9 | 610361 | ? | 13q33.1-q34 |
| OFC10 | 601912 | SUMO1 | 2q32.2-q33 |
| OFC11 | 600625 | BMP4 | 14q22 |
| OFC12 | 612858 | ? | 8q24.3 |
Many genes associated with syndromic cases of cleft lip/palate (see above) have been identified to contribute to the incidence of isolated cases of cleft lip/palate. This includes in particular sequence variants in the genes IRF6, PVRL1 and MSX1.[45] The understanding of the genetic complexities involved in the morphogenesis of the midface, including molecular and cellular processes, has been greatly aided by research on animal models, including of the genes BMP4, SHH, SHOX2, FGF10 and MSX1.[45]
Environmental factors
[edit]Environmental influences may also cause, or interact with genetics to produce, orofacial clefts. An example of the link between environmental factors and genetics comes from a research on mutations in the gene PHF8. The research found that PHF8 encodes for a histone lysine demethylase,[46] and is involved in epigenetic regulation. The catalytic activity of PHF8 depends on molecular oxygen,[46] a factor considered important from reports on increased incidence of cleft lip/palate in mice that have been exposed to hypoxia early during pregnancy.[47]
Cleft lip and other congenital abnormalities have also been linked to maternal hypoxia caused by maternal smoking,[48] with the estimated attributable fraction of orofacial clefts due to smoking in early pregnancy being 6.1%. Orofacial clefts occur very early in pregnancy and so smoking cessation right after recognition of pregnancy is unlikely to reduce the exposure during the critical time period.[49]
Maternal alcohol use has also been linked to cleft lip and palate due to the effects on the cranial neural crest cells. The degree of the effect, however, is unknown and requires further research.[50] Some forms of maternal hypertension treatment have been linked to cleft lip and palate.[51] Other environmental factors that have been studied include seasonal causes (such as pesticide exposure); maternal diet and vitamin intake; retinoids (members of the vitamin A family); anticonvulsant drugs; nitrate compounds; organic solvents; parental exposure to lead; alcohol; cigarette use; and a number of other psychoactive drugs (e.g. cocaine, crack cocaine, heroin).
Current research continues to investigate the extent to which folic acid can reduce the incidence of clefting.[52] Folic acid alone or in combination with vitamins and minerals prevents neural tube defects but does not have a clear effect on cleft lip palate incidence.[53] The mechanism behind beneficial folate supplementation is due to folate playing a pivotal role in DNA synthesis and methylation and contributes to both development and gene expression.[54]
Diagnosis
[edit]Traditionally, the diagnosis is made at the time of birth by physical examination. Recent advances in prenatal diagnosis have allowed obstetricians to diagnose facial clefts in utero with ultrasonography.[55]
Clefts can also affect other parts of the face, such as the eyes, ears, nose, cheeks, and forehead. In 1976, Paul Tessier described fifteen lines of cleft. Most of these craniofacial clefts are even rarer and are frequently described as Tessier clefts using the numerical locator devised by Tessier.[56]
Classification
[edit]Cleft lip and cleft palate is an "umbrella term" for a collection of orofacial clefts. It includes clefting of the upper lip, the maxillary alveolus (dental arch), and the hard or soft palate, in various combinations. Proposed anatomic combinations include:[57]
- cleft lip
- cleft lip and alveolus
- cleft lip, alveolus, and palate
- cleft lip and palate (with an intact alveolus)
- cleft palate
Prenatal diagnosis
[edit]Cleft lip with or without palate is classified as the most common congenital birth defect. It has been noted that the prevalence of orofacial clefts varies by race. The highest number of cases have been recorded among Asians and Native Americans, followed by Europeans, Hispanics and African-Americans. The critical period for cleft development ranges from the 4th to the 12th week of intrauterine life. Clefts of the primary palate develop between the 4th and 7th weeks of intrauterine life, while clefts of the secondary palate develop between the 8th and 12th embryonic weeks.
Accurate evaluation of craniofacial malformations is usually possible with the ultrasound scan performed during pregnancy. This is however not a routine procedure according to the American Institute of Ultrasound in Medicine. The accuracy of ultrasonography for prenatal diagnosis of cleft lip +/- palate is dependent on the experience of the sonologist, maternal body type, foetal position, the amount of amniotic fluid and the type of cleft.
Prenatal diagnosis enables appropriate and timely education and discussion with parents by the cleft team. This helps improve the quality of treatment received by the child and improves quality of life.
An accurate prenatal diagnosis of the CLP anomaly is critical for establishing long-term treatment planning, prediction of treatment outcome, and discussion and education of the parent. Although there is no intrauterine treatment for CLP, both mother and child benefit from early diagnosis and education. A multidisciplinary team approach is now accepted as the standard of care in dealing with CLP patients.
The time period immediately after the diagnosis and the first year after the birth is most challenging for parents. A systematically planned treatment plan and support system will help assist parents. The ultimate aim is to help educate parents and create awareness so as to improve care provided for the child.[58]
Treatment
[edit]Cleft lip and palate is very treatable; however, the kind of treatment depends on the type and severity of the cleft.
Most children with a form of clefting are monitored by a cleft palate team or craniofacial team through young adulthood.[59] Care can be lifelong and are looked after by craniofacial cleft teams often consist of: cleft surgeons, orthodontists, speech and language therapists, restorative dentists, psychologists, ENT surgeons and audio-logical physicians.[60]: 255 Treatment procedures can vary between craniofacial teams. For example, some teams wait on jaw correction until the child is aged 10 to 12 (argument: growth is less influential as deciduous teeth are replaced by permanent teeth, thus saving the child from repeated corrective surgeries), while other teams correct the jaw earlier (argument: less speech therapy is needed than at a later age when speech therapy becomes harder). Within teams, treatment can differ between individual cases depending on the type and severity of the cleft.
Cleft lip
[edit]Within the first 2–3 months after birth, surgery is performed to close the cleft lip. While surgery to repair a cleft lip can be performed soon after birth, often the preferred age is at approximately 10 weeks of age, following the "rule of 10s" coined by surgeons Wilhelmmesen and Musgrave in 1969 (the child is at least 10 weeks of age; weighs at least 10 pounds (4.5 kg), and has at least 10g/dL hemoglobin).[61][62] If the cleft is bilateral and extensive, two surgeries may be required to close the cleft, one side first, and the second side a few weeks later. The most common procedure to repair a cleft lip is the Millard procedure pioneered by Ralph Millard. Millard performed the first procedure at a Mobile Army Surgical Hospital (MASH) unit in Korea.[63]
Often an incomplete cleft lip requires the same surgery as complete cleft. This is done for two reasons. Firstly the group of muscles required to purse the lips run through the upper lip. To restore the complete group a full incision must be made. Secondly, to create a less obvious scar the surgeon tries to line up the scar with the natural lines in the upper lip (such as the edges of the philtrum) and tuck away stitches as far up the nose as possible. Incomplete cleft gives the surgeon more tissue to work with, creating a more supple and natural-looking upper lip.
-
 The blue lines indicate incisions.
The blue lines indicate incisions. -
 Movement of the flaps; flap A is moved between B and C. C is rotated slightly while B is pushed down.
Movement of the flaps; flap A is moved between B and C. C is rotated slightly while B is pushed down. -
 Pre-operation
Pre-operation -
 Post-operation, the lip is swollen from surgery and will look more natural within weeks. See photos in the section above.
Post-operation, the lip is swollen from surgery and will look more natural within weeks. See photos in the section above.




Pre-surgical devices
[edit]In some cases of a severe bilateral complete cleft, the premaxillary segment will be protruded far outside the mouth.
Nasoalveolar molding prior to surgery can improve long-term nasal symmetry where there is complete unilateral cleft lip–cleft palate, compared to correction by surgery alone, according to a retrospective cohort study.[64] In this study, significant improvements in nasal symmetry were observed in multiple areas including measurements of the projected length of the nasal ala (lateral surface of the external nose), position of the superoinferior alar groove, position of the mediolateral nasal dome, and nasal bridge deviation. "The nasal ala projection length demonstrated an average ratio of 93.0 percent in the surgery-alone group and 96.5 percent in the nasoalveolar molding group," this study concluded. A systematic review found in conclusion that nasoalveolar molding had a positive effect on the primary surgery of cleft lip/or palate treatment and aesthetics.[65]
Cleft palate
[edit]
Often a cleft palate is temporarily covered by a palatal obturator (a prosthetic device made to fit the roof of the mouth covering the gap). This device re-positions displaced alveolar segments and helps reduce the cleft lip separation. The obturator will improve speech as there's now proper airflow and improve feeding and breathing as the gap in the hard and soft palate is closed over so cannot affect it.[60]: 257
Cleft palate can also be corrected by surgery, usually performed between 6 and 12 months. Approximately 20–25% only require one palatal surgery to achieve a competent velopharyngeal valve capable of producing normal, non-hypernasal speech. However, combinations of surgical methods and repeated surgeries are often necessary as the child grows. One of the new innovations of cleft lip and cleft palate repair is the Latham appliance.[66] The Latham is surgically inserted by use of pins during the child's fourth or fifth month. After it is in place, the doctor, or parents, turn a screw daily to bring the cleft together to assist with future lip or palate repair.
If the cleft extends into the maxillary alveolar ridge, the gap is usually corrected by filling the gap with bone tissue. The bone tissue can be acquired from the individual's own chin, rib or hip.
At age 1–7 years the child is regularly reviewed by the cleft team.[60]: 257
Age 7–12 years, for the children born with alveolar clefts, they may need to have a secondary alveolar bone graft. This is where autogenous cancellous bone from a donor site (often the pelvic bone) is transplanted into the alveolar cleft region. This transplant of bone will close the osseous cleft of the alveolus, close any oro-nasal fistulae and will become integrated with the maxillary bone. It provides bone for teeth to erupt into and to allow implants to be placed as a possible future treatment option. The procedure should be carried out before the upper canine has erupted. Ideally the root of the canine should be one to two-thirds formed and that there is a space available to place the bone graft. Radio-graphs are taken to determine the quantity of missing bone in the cleft area.[60]: 258
Other surgeries
[edit]Orthognathic surgery – surgical cutting of bone to realign the upper jaw (osteotomy). The bone is cut then re-positioned and held together by wires or rigid fixation plates to ensure there's no anterior-posterior discrepancy, also to reduce scarring as it reduces growth. Single piece or multi-piece osteotomy exist. Single piece osteotomy is carried out where there is sufficient alveolar continuity achieved from a successful bone graft. Multi piece osteotomy is performed when there is a notable residual alveolar defect with a dental gap and oronasal fistula (communication between the oral and nasal cavities). The goal of both single and multi piece osteotomy is to displace the maxilla forward to obtain adequate occlusion as well to provide better support for upper lip and the nose and to close any fistulae.[67]
Distraction osteogenesis – bone lengthening by gradual distraction. This involves cutting bone and moving ends apart incrementally to allow new bone to form in the gap. This consists of several phases. After attachment of the distracting device and the bone cuts, there is a latency phase of 3–7 days when a callus forms. In the activation phase distraction of the callus induces bony ingrowth which can last up to 15 days depending on the required distraction. Once the required bone length is reached, the distraction device is left to remain in situ as it acts as a rigid skeletal fixation device until the new bone has matured (known as the consolidation period).[67]
Speech
[edit]Velopharyngeal insufficiency (VPI) can occur as a result of an unrepaired or repaired cleft lip and palate. VPI is the inability of the soft palate to close tightly against the back of the throat during speech, resulting in incomplete velopharyngeal closure. In turn, this results in speech abnormalities. Velopharyngeal closure is necessary during speech because it forms a seal between the nose and mouth, allowing the production of normal speech sounds. VPI can cause hypernasality (excessive nasal resonance), hyponasality (reduced nasal resonance), or a mixed nasal resonance, which is when hypernasality and hyponasality occur simultaneously.[68] In addition, CLP may cause abnormal positioning of individual teeth, which can in turn affect the patient's ability to make certain sounds when speaking such as the "f" or "v" sound and can also result in a lisp. The changes in speech may also be a manifestation on CLP's effects on the patient's occlusion.[16][17]
Hearing
[edit]Children with cleft palate have a very high risk of developing a middle ear infection, specifically otitis media. This is due to the immature development of the different bones and muscles in the ear. Otitis media is caused by the obstruction of the Eustachian tube, negative middle ear pressure and fluid build-up in the normally air-filled space of the middle ear.[69] This is associated with hearing impairment or loss. The insertion of a ventilation tube into the eardrum is a surgical treatment option commonly used to improve hearing in children with otitis media.[70] In addition, breast milk has been proven to decrease the incidence of otitis media in infants with clefts.[16]
Feeding
[edit]There are different options on how to feed a baby with cleft lip or cleft palate, including breast-feeding, bottle feeding, spoon feeding, and syringe feeding. Although breast-feeding is challenging, it improves weight-gain compared to spoon-feeding.[71] Nasal regurgitation is common due to the open space between the oral cavity and the nasal cavity. Bottle feeding can help (with squeezable bottles being easier to use than rigid bottles). In addition, maxillary plates can be added to aid in feeding. Whatever feeding method is established, it is important to keep the baby's weight gain and hydration monitored. Infants with cleft lip or palate may require supplemental feeds for adequate growth and nutrition. Breast feeding position as suggested by specialists can also improve success rate.[72]
Breast-feeding
[edit]Babies with cleft lip are more likely to breastfeed successfully than those with cleft palate and cleft lip and palate. Larger clefts of the soft or hard palate may not be able to generate suction as the oral cavity cannot be separated from the nasal cavity when feeding which leads to fatigue, prolonged feeding time, impaired growth and nutrition. Changes in swallowing mechanics may result in coughing, choking, gagging and nasal regurgitation. Even after cleft repair, the problem may still persist as significant motor learning of swallowing and sucking was absent for many months before repair.[73] These difficulties in feeding may result in secondary problems such as poor weight gain, excessive energy expenditure during feeding, lengthy feeding times, discomfort during feeding, and stressful feeding interactions between the infant and the mother. A potential source of discomfort for the baby during or after feeding is bloating or frequent "spit up" which is due to the excessive air intake through the nose and mouth in the open cleft.[16] Babies with cleft lip and or palate should be evaluated individually taking into account the size and location of the cleft and the mother's previous experience with breastfeeding.[71]
Another option is feeding breast milk via bottle or syringe. Since babies with clip lip and cleft palate generate less suction when breastfeeding, their nutrition, hydration and weight gain may be affected. This may result in the need for supplemental feeds. Modifying the position of holding the baby may increase the effectiveness and efficiency of breastfeeding.
Alternative feeding methods
[edit]Preoperative feeding – using a squeezable bottle instead of a rigid bottle can allow a higher volume of food intake and less effort to extract food. Using a syringe is practical, easy to perform and allows greater administered volume of food. It also means there will be weight gain and less time spent feeding.[74]
Post-operative feeding (isolated lip repair, or lip repair associated or not with palatoplasty) – post palatoplasty, some studies believe that inappropriate negative pressure on the suture line may affect results. Babies can be fed by a nasogastric tube instead. Studies suggest babies required less analgesics and shorter hospital stay with nasogastric feeding post-surgery. With bottle-feeding, there was higher feeding rejection and pain and required more frequent and prolonged feeding times.[74]
Treatment schedule
[edit]Each person's treatment schedule is individualized. The table below shows a common sample treatment schedule. The colored squares indicate the average timeframe in which the indicated procedure occurs. In some cases, this is usually one procedure, for example lip repair. In other cases, it is an ongoing therapy, for example speech therapy. In most cases of cleft lip and palate that involve the alveolar bone, patients will need a treatment plan including the prevention of cavities, orthodontics, alveolar bone grafting, and possibly jaw surgery.[75]
| Age | 0m
|
3m
|
6m
|
9m
|
1y
|
2y
|
3y
|
4y
|
5y
|
6y
|
7y
|
8y
|
9y
|
10y
|
11y
|
12y
|
13y
|
14y
|
15y
|
16y
|
17y
|
18y
|
| Palatal obturator | ||||||||||||||||||||||
| Repair cleft lip | ||||||||||||||||||||||
| Repair soft palate | ||||||||||||||||||||||
| Repair hard palate | ||||||||||||||||||||||
| Tympanostomy tube | ||||||||||||||||||||||
| Speech therapy/pharyngoplasty | ||||||||||||||||||||||
| Alveolar cleft grafting | ||||||||||||||||||||||
| Orthodontics | ||||||||||||||||||||||
| Orthognathic surgery |
Cleft team
[edit]People with CLP present with a multiplicity of problems. Therefore, effective management of CLP involves a wide range of specialists. The current model for delivery of this care is the multidisciplinary cleft team. This is a group of individuals from different specialist backgrounds who work closely together to provide patients with comprehensive care from birth through adolescence. This system of delivery of care enables the individuals within the team to function in an interdisciplinary way, so that all aspects of care for CLP patients can be provided in the best way possible.[76]
Outcomes assessment
[edit]Measuring the outcomes of CLP treatment has been laden with difficulty due to the complexity and longitudinal nature of cleft care, which spans birth through young adulthood. Prior attempts to study the effectiveness of specific interventions or overall treatment protocols have been hindered by a lack of data standards for outcomes assessment in cleft care.[citation needed]
The International Consortium for Health Outcome Measurement (ICHOM) has proposed the Standard Set of Outcome Measures for Cleft Lip and Palate.[77][78] The ICHOM Standard Set includes measures for many of the important outcome domains in cleft care (hearing, breathing, eating/drinking, speech, oral health, appearance and psychosocial well-being). It includes clinician-reported, patient-reported, and family-reported outcome measures.
Epidemiology
[edit]Cleft lip and palate occurs in about 1 to 2 per 1000 births in the developed world.[2]
Rates for cleft lip with or without cleft palate and cleft palate alone varies within different ethnic groups.
According to CDC, the prevalence of cleft palate in the United States is 6.35/10000 births and the prevalence of cleft lip with or without cleft palate is 10.63/10000 births.[79] The highest prevalence rates for cleft lip, either with or without cleft palate are reported for Native Americans and Asians. Africans have the lowest prevalence rates.[80]
- Native Americans: 3.74/1000
- Japanese: 0.82/1000 to 3.36/1000
- Chinese: 1.45/1000 to 4.04/1000
- White Americans: 1.43/1000 to 1.86/1000
- Latin Americans: 1.04/1000
- Africans: 0.18/1000 to 1.67/1000
Cleft lip and cleft palate caused about 3,800 deaths globally in 2017, down from 14,600 deaths in 1990.[4]
Prevalence of "cleft uvula" has varied from 0.02% to 18.8% with the highest numbers found among Chippewa and Navajo and the lowest generally in Africans.[81][82]
In 2025, the American Cleft Palate-Craniofacial Association (ACPA) put out an official statement related to epidemiology of cleft lip/palate in the United States:
APCA has long cited statistics of cleft prevalence as 7,000 children born in the United States each year, or 1 in 600 births. Several agencies collect this type of data, most notably the National Birth Defects Prevention Network (NBDPN). ... Even as global numbers vary in reported data, ACPA sought updated U.S.-specific data to provide a clearer understanding of U.S. prevalence. In 2023, data were compiled from reported state-specific departments of health for the years 2016-2020, and NBDPN published updated numbers in their birth defects reports.[83] No other update had been provided since the release of 2014 data. Therefore, ACPA recommends that healthcare and patient-advocacy organizations adopt the following statement regarding cleft prevalence in the United States:
"Between 6,000 and 8,000 children are born yearly in the United States with a cleft lip and/or palate. In the United States, about 1 in 1,050 babies is born with cleft lip with or without cleft palate, and about 1 in 1,600 babies is born with cleft palate alone." [84]
The CDC corroborates these new statistics and has updated its main cleft lip/palate web site, accordingly.[85]
Society and culture
[edit]
Handicap law and abortion controversies
[edit]In some countries, cleft lip or palate deformities are considered reasons (either generally tolerated or officially sanctioned) to perform an abortion beyond the legal fetal age limit, even though the fetus is not in jeopardy of life or limb.[86][87] Some political opponents contend this practice amounts to eugenics based on cosmetic defects rather than practical definitions of a disability.[88]
Works of fiction
[edit]The eponymous hero of J. M. Coetzee's 1983 novel Life & Times of Michael K has a cleft lip that is never corrected. In the 1920 novel Growth of the Soil, by Norwegian writer Knut Hamsun, Inger (wife of the main character) has an uncorrected cleft lip which puts heavy limitations on her life, even causing her to kill her own child, who is also born with a cleft lip. The protagonist of the 1924 novel Precious Bane, by English writer Mary Webb, is a young woman living in 19th-century rural Shropshire who eventually comes to feel that her deformity is the source of her spiritual strength. The book was later adapted for television by both the BBC and ORTF in France. Similarly, the main character in Graham Greene's 1936 crime noir novel A Gun for Sale, Raven, has a cleft lip which he is sensitive about, and is described as "an ugly man dedicated to ugly deeds". In the 1976 Patricia A. McKillip novel The Night Gift, one of the high-school aged protagonists is shy because she has a cleft lip, but learns to have more confidence in herself.
In the first edition of Harry Potter and the Chamber of Secrets, one of the people Gilderoy Lockhart stole credit from was a witch with a harelip who banished the Bandon Banshee. In later editions, this was changed to a witch with a hairy chin.[89]
In chapter 26 of Mark Twain's The Adventures of Huckleberry Finn, Huck Finn meets the three Wilks sisters, Mary Jane, Susan, and Joanna. Joanna is described as, "the one who gives herself to good works and has a hare-lip." As a form of offensive synecdoche, Huck Finn refers to Joanna as "the hare-lip" rather than by her name.
Cleft lip and cleft palate are often portrayed negatively in popular culture. Examples include Oddjob, the secondary villain of the James Bond novel Goldfinger by Ian Fleming (the film adaptation does not mention this but leaves it implied) and serial killer Francis Dolarhyde in the novel Red Dragon and its screen adaptations, Manhunter, Red Dragon, and Hannibal.[90] The portrayal of enemy characters with cleft lips and cleft palates, dubbed mutants, in the 2019 video game Rage 2 left Chris Plante of Polygon wondering if the condition would ever be portrayed positively.[91][92]
Some more ambiguous or positive portrayals include the minor character Johnny, a benign Slavic ancestor spirit, from the Witcher 3.[93] The actor Franz Rogowski, known for co-starring in the film Bird, has cleft.
Notable cases
[edit]| Name | Comments | |
|---|---|---|
| Jerry Byrd | American sportswriter for the Shreveport Journal, 1957–1991, and Bossier Press-Tribune, 1993–2012; born with cleft lip and without cleft palate | [94] |
| John Henry "Doc" Holliday | American dentist, gambler and gunfighter of the American Old West, who is usually remembered for his friendship with Wyatt Earp and the Gunfight at the O.K. Corral | [95] |
| Tutankhamen | Egyptian pharaoh who may have had a slightly cleft palate according to diagnostic imaging | [96] |
| Thorgils Skarthi | Thorgils 'the hare-lipped'—a 10th-century Viking warrior and founder of Scarborough, England. | [97] |
| Tad Lincoln | Fourth and youngest son of President Abraham Lincoln | [98] |
| Carmit Bachar | American dancer and singer | [99][100] |
| Jürgen Habermas | German philosopher and sociologist | [101] |
| Ljubo Milicevic | Australian professional footballer | [102] |
| Stacy Keach | American actor and narrator | [103] |
| Cheech Marin | American actor and comedian | [104] |
| Owen Schmitt | American football fullback | [105] |
| Tim Lott | English author and journalist | [106] |
| Richard Hawley | English musician | [106] |
| Dario Šarić | Croatian professional basketball player | [107] |
| Antoinette Bourignon | Flemish mystic | [108] |
| Tom Burke | English actor | [109] |
| Franz Rogowski | German actor | [110] |
| Aditya Chopra | Film director Producer Screen writer Studio executive | [111] |
Other animals
[edit]Cleft lips and palates are occasionally seen in cattle and dogs, and rarely in goats, sheep, cats, horses, pandas and ferrets. Most commonly, the defect involves the lip, rhinarium, and premaxilla. Clefts of the hard and soft palate are sometimes seen with a cleft lip. The cause is usually hereditary. Brachycephalic dogs such as Boxers and Boston Terriers are most commonly affected.[112] An inherited disorder with incomplete penetrance has also been suggested in Shih tzus, Swiss Sheepdogs, Bulldogs, and Pointers.[113] In horses, it is a rare condition usually involving the caudal soft palate.[114] In Charolais cattle, clefts are seen in combination with arthrogryposis, which is inherited as an autosomal recessive trait. It is also inherited as an autosomal recessive trait in Texel sheep. Other contributing factors may include maternal nutritional deficiencies, exposure in utero to viral infections, trauma, drugs, or chemicals, or ingestion of toxins by the mother, such as certain lupines by cattle during the second or third month of gestation.[115] The use of corticosteroids during pregnancy in dogs and the ingestion of Veratrum californicum by pregnant sheep have also been associated with cleft formation.[116]
Difficulty with nursing is the most common problem associated with clefts, but aspiration pneumonia, regurgitation, and malnutrition are often seen with cleft palate and is a common cause of death. Providing nutrition through a feeding tube is often necessary, but corrective surgery in dogs can be done by the age of twelve weeks.[112] For cleft palate, there is a high rate of surgical failure resulting in repeated surgeries.[117] Surgical techniques for cleft palate in dogs include prosthesis, mucosal flaps, and microvascular free flaps.[118] Affected animals should[opinion] not be bred due to the hereditary nature of this condition.[citation needed]
-
 Cleft lip in a Boxer
Cleft lip in a Boxer -
 Cleft lip in a Boxer with premaxillary involvement
Cleft lip in a Boxer with premaxillary involvement -
 Same dog as picture on left, one year later
Same dog as picture on left, one year later



See also
[edit]References
[edit]- ^ a b c d e f g h i j k l m n o p q r s t u "Facts about Cleft Lip and Cleft Palate". October 20, 2014. Archived from the original on May 8, 2015. Retrieved May 8, 2015.
- ^ a b c d e f Watkins SE, Meyer RE, Strauss RP, Aylsworth AS (April 2014). "Classification, epidemiology, and genetics of orofacial clefts". Clinics in Plastic Surgery. 41 (2): 149–163. doi:10.1016/j.cps.2013.12.003. PMID 24607185.
- ^ a b Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. (GBD 2017 Causes of Death Collaborators) (November 2018). "Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017". Lancet. 392 (10159): 1736–1788. doi:10.1016/S0140-6736(18)32203-7. PMC 6227606. PMID 30496103.
- ^ a b "GBD Results Tool | GHDx". ghdx.healthdata.org. Retrieved August 2, 2019.
- ^ Boklage CE (2010). How new humans are made cells and embryos, twins and chimeras, left and right, mind/selfsoul, sex, and schizophrenia. Singapore: World Scientific. p. 283. ISBN 978-981-283-514-7. Archived from the original on September 10, 2017.
- ^ Kim EK, Khang SK, Lee TJ, Kim TG (May 2010). "Clinical features of the microform cleft lip and the ultrastructural characteristics of the orbicularis oris muscle". The Cleft Palate-Craniofacial Journal. 47 (3): 297–302. doi:10.1597/08-270.1. PMID 19860522. S2CID 71448247.[permanent dead link]
- ^ Yuzuriha S, Mulliken JB (November 2008). "Minor-form, microform, and mini-microform cleft lip: anatomical features, operative techniques, and revisions". Plastic and Reconstructive Surgery. 122 (5): 1485–1493. doi:10.1097/PRS.0b013e31818820bc. PMID 18971733. S2CID 8551875.
- ^ Tosun Z, Hoşnuter M, Sentürk S, Savaci N (2003). "Reconstruction of microform cleft lip". Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery. 37 (4): 232–235. doi:10.1080/02844310310016412. PMID 14582757. S2CID 40850672.
- ^ Tollefson TT, Humphrey CD, Larrabee WF, Adelson RT, Karimi K, Kriet JD (2011). "The spectrum of isolated congenital nasal deformities resembling the cleft lip nasal morphology". Archives of Facial Plastic Surgery. 13 (3): 152–160. doi:10.1001/archfacial.2011.26. PMID 21576661.
- ^ a b Sloan GM (March 2000). "Posterior pharyngeal flap and sphincter pharyngoplasty: the state of the art". The Cleft Palate-Craniofacial Journal. 37 (2): 112–122. doi:10.1597/1545-1569(2000)037<0112:PPFASP>2.3.CO;2. PMID 10749049.
- ^ Hill JS (2001). "Velopharyngeal insufficiency: An update on diagnostic and surgical techniques". Current Opinion in Otolaryngology & Head and Neck Surgery. 9 (6): 365–8. doi:10.1097/00020840-200112000-00005. S2CID 76256148.
- ^ Kaplan EN (October 1975). "The occult submucous cleft palate". The Cleft Palate Journal. 12: 356–368. PMID 1058746.
- ^ Hanny KH, de Vries IA, Haverkamp SJ, Oomen KP, Penris WM, Eijkemans MJ, et al. (January 2016). "Late detection of cleft palate". European Journal of Pediatrics. 175 (1): 71–80. doi:10.1007/s00431-015-2590-9. PMC 4709386. PMID 26231683.
- ^ "Cleft Lip and Palate". American-Speech-Language-Hearing Association. Retrieved May 9, 2019.
- ^ "Index", Orthodontics: Principles and Practice, John Wiley & Sons, Ltd,., August 23, 2013, pp. 355–370, doi:10.1002/9781118785041.index, ISBN 978-1-118-78504-1
- ^ a b c d Goel S (2015). Feeding in Cleft Lip And Cleft Palata Infants. Saarbrücken, Germany: LAP LAMBERT Academic Publishing. pp. 20–22. ISBN 978-3-659-38212-3.
- ^ a b c Peterson-Falzone SJ, Trost-Cardamone JE, Karnell MP, Hardin-Jones MA (September 21, 2016). The clinician's guide to treating cleft palate speech (Second ed.). St. Louis, Missouri: Elsevier. ISBN 978-0-323-33934-6. OCLC 936145822.
- ^ Roberts RM, Mathias JL, Wheaton P (August 2012). "Cognitive functioning in children and adults with nonsyndromal cleft lip and/or palate: a meta-analysis". Journal of Pediatric Psychology. 37 (7): 786–797. doi:10.1093/jpepsy/jss052. PMID 22451260.
- ^ Leonard BJ, Brust JD, Abrahams G, Sielaff B (October 1991). "Self-concept of children and adolescents with cleft lip and/or palate". The Cleft Palate-Craniofacial Journal. 28 (4): 347–353. doi:10.1597/1545-1569(1991)028<0347:SCOCAA>2.3.CO;2. PMID 1742302.
- ^ Al-Namankany A, Alhubaishi A (August 2018). "Effects of cleft lip and palate on children's psychological health: A systematic review". Journal of Taibah University Medical Sciences. 13 (4): 311–318. doi:10.1016/j.jtumed.2018.04.007. PMC 6694901. PMID 31435341.
- ^ Hunt O, Burden D, Hepper P, Johnston C (June 2005). "The psychosocial effects of cleft lip and palate: a systematic review". European Journal of Orthodontics. 27 (3): 274–285. doi:10.1093/ejo/cji004. PMID 15947228.
- ^ Tobiasen JM (July 1984). "Psychosocial correlates of congenital facial clefts: a conceptualization and model". The Cleft Palate Journal. 21 (3): 131–139. PMID 6592056.
- ^ Pope AW, Ward J (September 1997). "Self-perceived facial appearance and psychosocial adjustment in preadolescents with craniofacial anomalies". The Cleft Palate-Craniofacial Journal. 34 (5): 396–401. doi:10.1597/1545-1569(1997)034<0396:SPFAAP>2.3.CO;2. PMID 9345606.
- ^ Bristow & Bristow 2007, pp. 82–92
- ^ "Cleft Palate Foundation". Archived from the original on July 1, 2007. Retrieved July 1, 2007.
- ^ Snyder HT, Bilboul MJ, Pope AW (September 2005). "Psychosocial adjustment in adolescents with craniofacial anomalies: a comparison of parent and self-reports". The Cleft Palate-Craniofacial Journal. 42 (5): 548–555. CiteSeerX 10.1.1.624.1274. doi:10.1597/04-078R.1. PMID 16149838. S2CID 37357550.
- ^ Endriga MC, Kapp-Simon KA (January 1999). "Psychological issues in craniofacial care: state of the art". The Cleft Palate-Craniofacial Journal. 36 (1): 3–11. doi:10.1597/1545-1569(1999)036<0001:PIICCS>2.3.CO;2. PMID 10067755.
- ^ a b Pope AW, Snyder HT (July 2005). "Psychosocial adjustment in children and adolescents with a craniofacial anomaly: age and sex patterns". The Cleft Palate-Craniofacial Journal. 42 (4): 349–354. doi:10.1597/04-043R.1. PMID 16001914. S2CID 31313562.
- ^ Prokhorov AV, Perry CL, Kelder SH, Klepp KI (1993). "Lifestyle values of adolescents: results from Minnesota Heart Health Youth Program". Adolescence. 28 (111): 637–647. PMID 8237549.
- ^ a b Dudas M, Li WY, Kim J, Yang A, Kaartinen V (2007). "Palatal fusion - where do the midline cells go? A review on cleft palate, a major human birth defect". Acta Histochemica. 109 (1): 1–14. doi:10.1016/j.acthis.2006.05.009. PMID 16962647.
- ^ a b Meeks NJ, Saenz M, Tsai AC, Elias ER (2018). "Genetics & Dysmorphology". In Hay WW, Levin MJ, Deterding RR, Abzug MJ (eds.). Current Diagnosis & Treatment: Pediatrics (24th ed.). McGraw-Hill Education. Retrieved August 6, 2019.
- ^ Beaty TH, Ruczinski I, Murray JC, Marazita ML, Munger RG, Hetmanski JB, et al. (September 2011). "Evidence for gene-environment interaction in a genome wide study of nonsyndromic cleft palate". Genetic Epidemiology. 35 (6): 469–478. doi:10.1002/gepi.20595. PMC 3180858. PMID 21618603.
- ^ Kanno K, Suzuki Y, Yamada A, Aoki Y, Kure S, Matsubara Y (May 2004). "Association between nonsyndromic cleft lip with or without cleft palate and the glutamic acid decarboxylase 67 gene in the Japanese population". American Journal of Medical Genetics. Part A. 127A (1): 11–16. doi:10.1002/ajmg.a.20649. PMID 15103710. S2CID 30016360.
- ^ Sandoiu A (January 17, 2017). "Scientists find genetic mutation that causes cleft lip and palate, heart defects". Medical News Today. Archived from the original on January 29, 2017. Retrieved January 31, 2017.
- ^ Dixon MJ, Marazita ML, Beaty TH, Murray JC (March 2011). "Cleft lip and palate: understanding genetic and environmental influences". Nature Reviews. Genetics. 12 (3): 167–178. doi:10.1038/nrg2933. PMC 3086810. PMID 21331089.
- ^ Zucchero TM, Cooper ME, Maher BS, Daack-Hirsch S, Nepomuceno B, Ribeiro L, et al. (August 2004). "Interferon regulatory factor 6 (IRF6) gene variants and the risk of isolated cleft lip or palate". The New England Journal of Medicine. 351 (8): 769–780. doi:10.1056/NEJMoa032909. PMID 15317890. S2CID 3324418.
- ^ "Cleft palate genetic clue found". BBC News. August 30, 2004. Archived from the original on February 8, 2007. Retrieved July 1, 2007.
- ^ Kousa YA, Zhu H, Fakhouri WD, Lei Y, Kinoshita A, Roushangar RR, et al. (May 2019). "The TFAP2A-IRF6-GRHL3 genetic pathway is conserved in neurulation". Human Molecular Genetics. 28 (10): 1726–1737. doi:10.1093/hmg/ddz010. PMC 6494790. PMID 30689861.
- ^ Siderius LE, Hamel BC, van Bokhoven H, de Jager F, van den Helm B, Kremer H, et al. (July 1999). "X-linked mental retardation associated with cleft lip/palate maps to Xp11.3-q21.3". American Journal of Medical Genetics. 85 (3): 216–220. doi:10.1002/(SICI)1096-8628(19990730)85:3<216::AID-AJMG6>3.0.CO;2-X. PMID 10398231.
- ^ Kronwith SD, Quinn G, McDonald DM, Cardonick E, Onyx P, LaRossa D, et al. (1990). "Stickler's syndrome in the Cleft Palate Clinic". Journal of Pediatric Ophthalmology and Strabismus. 27 (5): 265–267. doi:10.3928/0191-3913-19900901-12. PMID 2246742.
- ^ Mrugacz M, Sredzińska-Kita D, Bakunowicz-Lazarczyk A, Piszcz M (2005). "[High myopia as a pathognomonic sign in Stickler's syndrome]". Klinika Oczna (in Polish). 107 (4–6): 369–371. PMID 16118961.
- ^ Sousa SB, Lambot-Juhan K, Rio M, Baujat G, Topouchian V, Hanna N, et al. (May 2011). "Expanding the skeletal phenotype of Loeys-Dietz syndrome". American Journal of Medical Genetics. Part A. 155A (5): 1178–1183. doi:10.1002/ajmg.a.33813. PMID 21484991. S2CID 27999412.
- ^ Hardikar syndrome symptoms
- ^ Wall J, Albanese CT (2015), Doherty GM (ed.), "Pediatric Surgery", CURRENT Diagnosis & Treatment: Surgery (14th ed.), McGraw-Hill Education, retrieved August 6, 2019
- ^ a b Cox TC (March 2004). "Taking it to the max: the genetic and developmental mechanisms coordinating midfacial morphogenesis and dysmorphology". Clinical Genetics. 65 (3): 163–176. doi:10.1111/j.0009-9163.2004.00225.x. PMID 14756664. S2CID 22472334.
- ^ a b Loenarz C, Ge W, Coleman ML, Rose NR, Cooper CD, Klose RJ, et al. (January 2010). "PHF8, a gene associated with cleft lip/palate and mental retardation, encodes for an Nepsilon-dimethyl lysine demethylase". Human Molecular Genetics. 19 (2): 217–222. doi:10.1093/hmg/ddp480. PMC 4673897. PMID 19843542.
- ^ Millicovsky G, Johnston MC (September 1981). "Hyperoxia and hypoxia in pregnancy: simple experimental manipulation alters the incidence of cleft lip and palate in CL/Fr mice". Proceedings of the National Academy of Sciences of the United States of America. 78 (9): 5722–5723. Bibcode:1981PNAS...78.5722M. doi:10.1073/pnas.78.9.5722. PMC 348841. PMID 6946511.
- ^ Shi M, Wehby GL, Murray JC (March 2008). "Review on genetic variants and maternal smoking in the etiology of oral clefts and other birth defects". Birth Defects Research. Part C, Embryo Today. 84 (1): 16–29. doi:10.1002/bdrc.20117. PMC 2570345. PMID 18383123.
- ^ Honein MA, Devine O, Grosse SD, Reefhuis J (November 2014). "Prevention of orofacial clefts caused by smoking: implications of the Surgeon General's report". Birth Defects Research. Part A, Clinical and Molecular Teratology. 100 (11): 822–825. doi:10.1002/bdra.23274. PMC 4559232. PMID 25045059.
- ^ Bell JC, Raynes-Greenow C, Turner RM, Bower C, Nassar N, O'Leary CM (July 2014). "Maternal alcohol consumption during pregnancy and the risk of orofacial clefts in infants: a systematic review and meta-analysis". Paediatric and Perinatal Epidemiology. 28 (4): 322–332. doi:10.1111/ppe.12131. PMID 24800624.
- ^ Hurst JA, Houlston RS, Roberts A, Gould SJ, Tingey WG (October 1995). "Transverse limb deficiency, facial clefting and hypoxic renal damage: an association with treatment of maternal hypertension?". Clinical Dysmorphology. 4 (4): 359–363. doi:10.1097/00019605-199510000-00013. PMID 8574428. S2CID 6330050.
- ^ Boyles AL, Wilcox AJ, Taylor JA, Meyer K, Fredriksen A, Ueland PM, et al. (February 2008). "Folate and one-carbon metabolism gene polymorphisms and their associations with oral facial clefts". American Journal of Medical Genetics. Part A. 146A (4): 440–449. doi:10.1002/ajmg.a.32162. PMC 2366099. PMID 18203168.
- ^ De-Regil LM, Peña-Rosas JP, Fernández-Gaxiola AC, Rayco-Solon P (December 2015). "Effects and safety of periconceptional oral folate supplementation for preventing birth defects". The Cochrane Database of Systematic Reviews. 2015 (12) CD007950. doi:10.1002/14651858.CD007950.pub3. PMC 8783750. PMID 26662928.
- ^ Wehby GL, Goco N, Moretti-Ferreira D, Felix T, Richieri-Costa A, Padovani C, et al. (November 2012). "Oral cleft prevention program (OCPP)". BMC Pediatrics. 12 (1) 184. doi:10.1186/1471-2431-12-184. PMC 3532199. PMID 23181832.
- ^ Costello BJ, Edwards SP, Clemens M (October 2008). "Fetal diagnosis and treatment of craniomaxillofacial anomalies". Journal of Oral and Maxillofacial Surgery. 66 (10): 1985–1995. doi:10.1016/j.joms.2008.01.042. PMID 18848093.
- ^ Tessier P (June 1976). "Anatomical classification facial, cranio-facial and latero-facial clefts". Journal of Maxillofacial Surgery. 4 (2): 69–92. doi:10.1016/S0301-0503(76)80013-6. PMID 820824.
- ^ Allori AC, Mulliken JB, Meara JG, Shusterman S, Marcus JR (March 2017). "Classification of Cleft Lip/Palate: Then and Now". The Cleft Palate-Craniofacial Journal. 54 (2): 175–188. doi:10.1597/14-080. PMID 26339868. S2CID 207236616.
- ^ Sreejith VP, Arun V, Devarajan AP, Gopinath A, Sunil M (2018). "Psychological Effect of Prenatal Diagnosis of Cleft Lip and Palate: A Systematic Review". Contemporary Clinical Dentistry. 9 (2): 304–308. doi:10.4103/ccd.ccd_673_17. PMC 5968700. PMID 29875578.
- ^ Bristow L, Bristow S (2007). Making faces: Logan's cleft lip and palate story. Oakville, Ontaria, CA: Pulsus Group. pp. 1–92.
- ^ a b c d Gill DS, Naini FB (2011). Orthodontics: Principles and Practice. p. 257.
- ^ Lydiatt DD, Yonkers AJ, Schall DG (November 1989). "The management of the cleft lip and palate patient". The Nebraska Medical Journal. 74 (11): 325–8, discussion 328–9. PMID 2586685.
- ^ Sriram Bhat M (2014). SRB's Surgical Operations: Text & Atlas. JP Medical Ltd. p. 414. ISBN 978-93-5025-121-8.
- ^ "Biography and Personal Archive". Archived from the original on June 17, 2007. Retrieved July 1, 2007. at miami.edu
- ^ Barillas I, Dec W, Warren SM, Cutting CB, Grayson BH (March 2009). "Nasoalveolar molding improves long-term nasal symmetry in complete unilateral cleft lip-cleft palate patients". Plastic and Reconstructive Surgery. 123 (3): 1002–1006. doi:10.1097/PRS.0b013e318199f46e. PMID 19319066. S2CID 24514123.
- ^ Maillard S, Retrouvey JM, Ahmed MK, Taub PJ (September 30, 2017). "Correlation between Nasoalveolar Molding and Surgical, Aesthetic, Functional and Socioeconomic Outcomes Following Primary Repair Surgery: a Systematic Review". Journal of Oral & Maxillofacial Research. 8 (3) e2. doi:10.5037/jomr.2017.8302. PMC 5676312. PMID 29142654.
- ^ Fukuyama E, Omura S, Fujita K, Soma K, Torikai K (November 2006). "Excessive rapid palatal expansion with Latham appliance for distal repositioning of protruded premaxilla in bilateral cleft lip and alveolus". The Cleft Palate-Craniofacial Journal. 43 (6): 673–677. doi:10.1597/05-109. PMID 17105324. S2CID 34126577.
- ^ a b Kloukos D, Fudalej P, Sequeira-Byron P, Katsaros C (August 2018). "Maxillary distraction osteogenesis versus orthognathic surgery for cleft lip and palate patients". The Cochrane Database of Systematic Reviews. 2018 (8) CD010403. doi:10.1002/14651858.CD010403.pub3. PMC 6513261. PMID 30095853.
- ^ Nasser M, Fedorowicz Z, Newton JT, Nouri M (January 2008). Nasser M (ed.). "Interventions for the management of submucous cleft palate". The Cochrane Database of Systematic Reviews (1) CD006703. doi:10.1002/14651858.CD006703.pub2. PMID 18254111.
- ^ Steele D, Adam GP, Di M, Halladay C, Pan I, Coppersmith N, et al. (2017). Tympanostomy Tubes in Children With Otitis Media. AHRQ Comparative Effectiveness Reviews. Rockville (MD): Agency for Healthcare Research and Quality (US). PMID 28817250.
- ^ Browning GG, Rovers MM, Williamson I, Lous J, Burton MJ (October 2010). "Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children". The Cochrane Database of Systematic Reviews (10) CD001801. doi:10.1002/14651858.CD001801.pub3. PMID 20927726. S2CID 43568574.
- ^ a b Reilly S, Reid J, Skeat J, Cahir P, Mei C, Bunik M (2013). "'ABM clinical protocol #18: guidelines for breastfeeding infants with cleft lip, cleft palate, or cleft lip and palate, revised 2013.', Academy of Breastfeeding Medicine" (PDF).
- ^ Matsunaka E, Ueki S, Makimoto K (October 2015). "Impact of breastfeeding or bottle-feeding on surgical wound dehiscence after cleft lip repair in infants: a systematic review protocol". JBI Database of Systematic Reviews and Implementation Reports. 13 (10): 3–11. doi:10.11124/jbisrir-2015-2336. PMID 26571277. S2CID 45396841.
- ^ Bessell A, Hooper L, Shaw WC, Reilly S, Reid J, Glenny AM (February 2011). "Feeding interventions for growth and development in infants with cleft lip, cleft palate or cleft lip and palate". The Cochrane Database of Systematic Reviews. 2011 (2) CD003315. John Wiley & Sons, Ltd. doi:10.1002/14651858.cd003315. hdl:10072/172084. PMC 7144736. PMID 21328261.
- ^ a b Duarte GA, Ramos RB, Cardoso MC (September 1, 2016). "Feeding methods for children with cleft lip and/or palate: a systematic review". Brazilian Journal of Otorhinolaryngology. 82 (5): 602–609. doi:10.1016/j.bjorl.2015.10.020. PMC 9444722. PMID 26997574.
- ^ Scalzone A, Flores-Mir C, Carozza D, d'Apuzzo F, Grassia V, Perillo L (February 2019). "Secondary alveolar bone grafting using autologous versus alloplastic material in the treatment of cleft lip and palate patients: systematic review and meta-analysis". Progress in Orthodontics. 20 (1) 6. doi:10.1186/s40510-018-0252-y. PMC 6369233. PMID 30740615.
- ^ Hodgkinson PD, Brown S, Duncan D, Grant C, McNaughton AM, Thomas P (February 2005). "Management of Children with Cleft Lip and Palate: A Review Describing the Application of Multidisciplinary Team Working in This Condition Based Upon the Experiences of a Regional Cleft Lip and Palate Centre in the United Kingdom". Fetal and Maternal Medicine Review. 16 (1): 1–27. CiteSeerX 10.1.1.483.9042. doi:10.1017/S0965539505001452. ISSN 1469-5065. S2CID 36404355.
- ^ "ICHOM | Cleft Lip & Palate Standard Set | Measuring Outcomes".
- ^ Allori AC, Kelley T, Meara JG, Albert A, Bonanthaya K, Chapman K, et al. (September 2017). "A Standard Set of Outcome Measures for the Comprehensive Appraisal of Cleft Care". The Cleft Palate-Craniofacial Journal. 54 (5): 540–554. doi:10.1597/15-292. PMID 27223626. S2CID 43371901.
- ^ "Prevalence of Cleft Lip & Cleft Palate | National Institute of Dental and Craniofacial Research". www.nidcr.nih.gov. Retrieved August 2, 2019.
- ^ See "Who is affected by cleft lip and cleft palate". Archived from the original on March 30, 2008. Retrieved June 20, 2008.
- ^ Cervenka J, Shapiro BL (February 1970). "Cleft uvula in Chippewa Indians: prevalence and genetics". Human Biology. 42 (1): 47–52. PMID 5445084.
- ^ Rivron RP (March 1989). "Bifid uvula: prevalence and association in otitis media with effusion in children admitted for routine otolaryngological operations". The Journal of Laryngology and Otology. 103 (3): 249–252. doi:10.1017/S002221510010862X. PMID 2784825. S2CID 32750501.
- ^ Stallings EB, Isenburg JL, Rutkowski RE, Kirby RS, Nembhard WN, Sandidge T, et al. (2024). "National population-based estimates for major birth defects, 2016–2020". Birth Defects Research. 116 (1) e2301. doi:10.1002/bdr2.2301. PMC 10898112. PMID 38277408.
- ^ "ACPA announcement".
- ^ "CDC Cleft Lip/Palate". December 26, 2024.
- ^ Dobson R (November 2003). "Review of abortion law demanded after abortion for cleft palate". BMJ. 327 (7426): 1250. doi:10.1136/bmj.327.7426.1250-c. PMC 1126893. PMID 14644964.
- ^ Hill, Amelia. "MPs bring bill to ban late abortions for cleft lip, cleft palate and clubfoot," The Guardian, 2020.
- ^ Allison R (December 2, 2003). "Does a cleft palate justify an abortion? Curate wins right to challenge doctors". The Guardian. ISSN 0261-3077. Retrieved September 13, 2024.
- ^ VanderArk S (June 6, 2017). "Edits and Changes to the Text of CS". The Harry Potter Lexicon. Retrieved September 12, 2020.
- ^ Harfield TD. "The Monster Without: Red Dragon, the Cleft-Lip, and the Politics of Recognition" (PDF). Archived from the original (PDF) on February 21, 2014. Retrieved February 5, 2014.
- ^ Plante C (June 14, 2018). "When I asked about Rage 2's worst character, I got an unexpected response". Polygon. Retrieved May 15, 2019.
- ^ Plante C (May 13, 2019). "Rage 2 is a fun game that makes me feel like garbage". Polygon. Retrieved May 15, 2019.
- ^ "Johnny". The Witcher Wiki. Retrieved October 31, 2025.
- ^ Nico Van Thyn (June 8, 2012). "Once a Knight: The legendary man, Mr. Byrd". nvanthyn.blogsport.com. Archived from the original on October 5, 2016. Retrieved April 22, 2016.
- ^ Tanner KH (1998). Doc Holliday: A Family Portrait. University of Omaha Press. ISBN 978-0-8061-3036-1.
- ^ "King Tut Not Murdered Violently, CT Scans Show". Archived from the original on July 3, 2007. Retrieved July 1, 2007.
- ^ Bloodfeud: Murder and Revenge in Anglo-Saxon England, Richard Fletcher
- ^ "Tad Lincoln: The Not-so-Famous Son of A Most-Famous President". HistoryBuff.com. Archived from the original on September 27, 2007. Retrieved July 1, 2007.
- ^ "Carmit Bachar, smile ambassador". October 13, 2007. Archived from the original on October 30, 2007. Retrieved October 13, 2007.
- ^ Beverley Lyons, October 16, 2006. Carmite Doing Her Bit For Charity Archived September 27, 2007, at the Wayback Machine. The Daily Record
- ^ "Jurgen Habermas". Retrieved December 18, 2008.
- ^ "Chat To Ljubo...LIVE". May 28, 2009. Archived from the original on May 31, 2009. Retrieved December 23, 2009.
- ^ "Stacy Keach". Cleft Palate Foundation. Archived from the original on February 13, 2007. Retrieved July 1, 2007.
- ^ "Cheech Marin". Cleft Palate Foundation. Retrieved July 1, 2007.
- ^ Whiteside K (November 4, 2006). "Schmitt is face of West Va. toughness| USA Today". Archived from the original on October 15, 2009. Retrieved April 30, 2010.
- ^ a b "Famous People with a Cleft". April 5, 2008. Archived from the original on January 21, 2013.
- ^ "Who's That Guy? Dario Saric!". September 3, 2014. Archived from the original on August 22, 2014.
- ^ MacEwen A (1910). Antoinette Bourignon, Quietist. London: Hodder and Stoughton. p. 27. Archived from the original on February 6, 2015. Retrieved May 15, 2015.
- ^ Cartwright G (September 30, 2017). "He Was Born With a Cleft Lip". POPSUGAR Celebrity UK. Archived from the original on June 30, 2019. Retrieved May 15, 2019.
- ^ Bartels G (February 18, 2018). "Franz Rogowski im Porträt – Schönheit des Makels". Der Tagesspiegel Online (in German). Retrieved February 6, 2021.
Dass ihm, der Hasenscharte, dem Lispeln und der hellen Stimme wegen auf der Bühne Grenzen gesetzt sind, ist ihm klar.
- ^ IMDB (February 18, 2025). "Aditya Chopra Travia – Imdb". Imdb. Retrieved February 6, 2025.
Aditya Chopra Travia.
- ^ a b Ettinger SJ, Feldman EC (1995). Textbook of Veterinary Internal Medicine (4th ed.). W.B. Saunders Company. ISBN 978-0-7216-6795-9.
- ^ Rodriguez Garcia JF (2006). "Surgery of the Soft and Hard Palate". Proceedings of the North American Veterinary Conference. Retrieved April 28, 2007.
- ^ Semevolos SA, Ducharme N (1998). "Surgical Repair of Congenital Cleft Palate in Horses: Eight Cases (1979–1997)" (PDF). Proceedings of the American Association of Equine Practitioners. Archived (PDF) from the original on September 29, 2007. Retrieved April 28, 2007.
- ^ "Mouth". The Merck Veterinary Manual. 2006. Archived from the original on September 29, 2007. Retrieved April 28, 2007.
- ^ Beasley, V. (1999). "Teratogenic Agents". Veterinary Toxicology. Archived from the original on September 20, 2004. Retrieved April 28, 2007.
- ^ Lee JI, Kim YS, Kim MJ, Lee J, Choi JH, Yeom DB, et al. (March 2006). "Application of a temporary palatal prosthesis in a puppy suffering from cleft palate". Journal of Veterinary Science. 7 (1): 93–95. doi:10.4142/jvs.2006.7.1.93. PMC 3242096. PMID 16434860.
- ^ Griffiths LG, Sullivan M (2001). "Bilateral overlapping mucosal single-pedicle flaps for correction of soft palate defects". Journal of the American Animal Hospital Association. 37 (2): 183–186. doi:10.5326/15473317-37-2-183. PMID 11300527.
Further reading
[edit]- FIGURE 1 | Development of the lip and palate and FIGURE 2 | Types of cleft in Dixon MJ, Marazita ML, Beaty TH, Murray JC (March 2011). "Cleft lip and palate: understanding genetic and environmental influences". Nature Reviews. Genetics. 12 (3): 167–178. doi:10.1038/nrg2933. PMC 3086810. PMID 21331089.
- Berkowitz S (February 26, 2013). Cleft Lip and Palate: Diagnosis and Management. Springer. ISBN 978-3-642-30770-6.
External links
[edit]Cleft lip and cleft palate
View on GrokipediaEmbryology and Pathogenesis
Normal facial development
The development of the human face occurs primarily between the 4th and 10th weeks of gestation, initiating with the formation of facial prominences around the stomodeum during the 4th week. These include the frontonasal prominence superiorly, paired maxillary prominences laterally, and mandibular prominences inferiorly, derived from neural crest mesenchyme and ectodermal interactions.[7] By the 5th week, nasal placodes invaginate within the frontonasal prominence to form medial and lateral nasal prominences, which grow toward the midline. Fusion of the medial nasal prominences with the ipsilateral maxillary prominences begins around the 6th week, establishing the philtrum and primary palate (intermaxillary segment), while lateral nasal prominences contribute to the nostrils.[8] This process requires precise medial migration and contact-dependent adhesion of epithelial-covered mesenchymal cores.[9] Cranial neural crest cells, originating from the dorsal neural tube between the 3rd and 4th weeks, migrate ventrally into the facial prominences, populating the mesenchyme that forms connective tissue, cartilage, and bone precursors of the maxilla and nasomaxillary structures. These cells provide the cellular substrate for growth and differentiation, with their spatiotemporal distribution ensuring balanced expansion of prominences.[10] Signaling pathways, including bone morphogenetic proteins (BMPs), fibroblast growth factors (FGFs), and Sonic hedgehog (SHH), orchestrate proliferation, survival, and patterning; for instance, BMP and SHH gradients in the frontonasal ectoderm regulate mesenchymal proliferation in the facial ectoderm zone (FEZ), directing bud outgrowth.[11] FGFs from the ectoderm promote mesenchymal proliferation, while SHH maintains epithelial integrity during fusion events.[12] The secondary palate develops concurrently from the 6th week, with lateral palatine processes (shelves) emerging from the maxillary prominences and initially oriented vertically alongside the tongue. Shelf elevation to a horizontal position occurs between weeks 7 and 8, involving hyoid-tongue descent, cytoskeletal remodeling, and extracellular matrix changes, followed by midline fusion by week 9.[8] Epithelial seam removal post-fusion relies on programmed cell death (apoptosis) in the midline epithelial cells, ensuring mesenchymal confluence without scarring.[13] Mouse models demonstrate this coordination, with high-resolution imaging revealing synchronized neural crest-derived mesenchymal expansion and epithelial signaling from embryonic day 10 to 14, underscoring the narrow temporal window for normal closure.[14]Mechanisms of cleft formation
Cleft lip results from the incomplete fusion of the medial nasal prominences with the ipsilateral maxillary prominences, which normally occurs between the 4th and 7th weeks of embryonic development. This process involves the outgrowth, approximation, and seamless merging of these facial prominences derived from the first branchial arch and frontonasal prominence, mediated by epithelial contact and subsequent mesenchymal bridging. Disruptions in cellular migration, proliferation, or apoptosis at the fusion interface can prevent this closure, leading to a spectrum of anterior defects ranging from microform notches to complete bilateral clefts extending through the alveolus.[8][1] In contrast, cleft palate primarily stems from failures in the development of the secondary palate, occurring later between the 6th and 12th weeks of gestation, after primary palate formation. The palatal shelves, outgrowths of the maxillary prominences, must elevate from a vertical to horizontal position over the tongue, apposed by tongue depression, before undergoing midline fusion via epithelial seam breakdown and mesenchymal confluence. Mechanical barriers, such as impaired shelf elevation due to tongue immobility or biochemical deficiencies in extracellular matrix remodeling, disrupt this sequence, resulting in posterior clefts isolated from or continuous with lip defects.[15][8] Histological examinations of human embryos and animal models reveal that fusion failures often involve persistent epithelial barriers or defective basement membrane rupture post-contact, as seen in disrupted transforming growth factor-beta signaling pathways. Knockout mouse models, such as those deficient in Esrp1 or TGFβ3, demonstrate halted shelf elevation or seam persistence, underscoring multifactorial etiologies including genetic perturbations in adhesion molecules and growth factors that impair proliferation and directed migration without single deterministic causes. These experimental disruptions mimic human cleft phenotypes, highlighting causal roles for both intrinsic cellular defects and extrinsic mechanical interferences in palatogenesis.[16][17][18]Syndromic versus nonsyndromic clefts
Cleft lip and/or palate (CL/P) cases are classified as nonsyndromic when occurring in isolation without associated congenital anomalies or recognized syndromes, comprising approximately 70% of CL/P instances and reflecting a multifactorial etiology involving polygenic inheritance and environmental influences.[19] In contrast, syndromic clefts, affecting about 30% of CL/P cases, manifest as components of broader genetic disorders featuring additional extracraniofacial or craniofacial malformations, often driven by monogenic mutations with high penetrance that elevate familial recurrence risks compared to the lower, empirically observed 3-5% sibling recurrence in nonsyndromic forms.[20][21] This distinction underscores a causal predominance of Mendelian inheritance in syndromic variants, where single-gene disruptions during embryogenesis precipitate both the cleft and syndromic features, as opposed to the threshold model of liability in nonsyndromic cases.[22] For isolated cleft palate (CP) without lip involvement, the syndromic proportion rises to roughly 50%, with nonsyndromic CP showing similar multifactorial patterns but heightened sensitivity to genetic-environmental thresholds.[19] Common syndromic examples include Van der Woude syndrome, the most frequent syndromic CL/P at 2% of total cases, characterized by autosomal dominant IRF6 mutations leading to lower lip pits alongside clefts and occasional popliteal pterygia.[21][23] Pierre Robin sequence, frequently syndromic and involving cleft palate with micrognathia and glossoptosis, often links to underlying connective tissue disorders like Stickler syndrome, necessitating evaluation for airway obstruction and skeletal anomalies that influence surgical timing and multidisciplinary management.[24] Diagnostic differentiation via clinical examination and genetic testing is critical, as syndromic cases demand screening for comorbidities like hearing loss or cardiac defects, altering prognosis through increased morbidity beyond the cleft itself.[25] Early identification mitigates risks, with syndromic forms exhibiting recurrence rates up to 50% in dominant patterns versus the population baseline.[22]Etiology
Genetic contributions
Twin studies demonstrate high heritability for nonsyndromic cleft lip with or without cleft palate (NSCL/P), with monozygotic concordance rates of 40-60% compared to 3-5% in dizygotic twins, yielding estimates of 70-90% genetic contribution after accounting for shared environments.[26][27] These findings refute models minimizing genetic influence, as the substantial difference in twin concordances indicates predominant polygenic inheritance over environmental dominance alone.[28] Family-based risks further underscore genetic loading, with sibling recurrence rates of 3-5% for NSCL/P in probands, rising to 9% or higher with multiple affected relatives, consistent with a multifactorial threshold model where cumulative genetic liability exceeds a population-specific threshold.[29][30] Genome-wide association studies (GWAS) support this by identifying over 40 risk loci explaining up to 40% of heritability, with polygenic risk scores (PRS) integrating these variants to predict case status more accurately than single-locus effects.[31][32] Key candidate genes include IRF6, variants of which disrupt transcription regulation critical for lip epithelial fusion during embryogenesis, conferring 12-20% population-attributable risk for NSCL/P across ancestries.[33] MSX1 mutations impair mesenchymal signaling in palatal shelf elevation and odontogenesis, linking cleft palate to associated tooth agenesis in familial cases.[34] FOXE1 polymorphisms affect both NSCL/P and isolated cleft palate by altering thyroid and craniofacial morphogenesis pathways, as validated in multi-ethnic cohorts.[35] Recent 2024 multi-ancestry GWAS meta-analyses confirm these associations while uncovering novel loci, emphasizing ethnic-specific allele frequencies without evidence of low-penetrance environmental overrides in genetic architecture.[36][37]Environmental risk factors
Maternal smoking during pregnancy is associated with an increased risk of nonsyndromic cleft lip with or without cleft palate (CL/P), with meta-analyses reporting odds ratios (OR) of approximately 1.2 to 1.5 overall, and higher for isolated cleft palate (OR 1.50, 95% CI 1.20-1.88).[38] [39] Dose-response relationships have been observed in cohort studies, where heavier smoking (e.g., >20 cigarettes per day) elevates risk up to twofold, likely due to nicotine-induced vasoconstriction and oxidative stress impairing vascular supply and cell migration during the critical 4- to 7-week embryonic window of facial development.[40] Passive smoke exposure shows weaker but positive associations in systematic reviews (OR ~1.1).[41] Pre-existing maternal diabetes, particularly pregestational type 1 or 2, confers an elevated risk for orofacial clefts, with adjusted ORs ranging from 1.35 (95% CI 1.00-1.82) to over 2-fold in population-based studies, independent of glycemic control in some analyses.[42] [38] Hyperglycemia disrupts embryogenic signaling pathways, such as sonic hedgehog, during gastrulation and neural crest cell migration, though absolute risks remain below 1% even among exposed pregnancies given baseline cleft prevalence of ~1 in 700 births. Gestational diabetes shows inconsistent links, with ORs near 1.0-1.5 but limited confounding adjustment.[43] Certain anticonvulsant medications, including phenytoin and valproate, are teratogenic, increasing cleft risk through interference with neural crest-derived mesenchyme proliferation; maternal exposure to phenytoin is linked to fetal hydantoin syndrome featuring cleft lip/palate in up to 10% of cases (3- to 10-fold relative risk), while valproate elevates overall malformation rates including clefts (OR ~5 for cleft palate).[44] [45] These effects are most pronounced with first-trimester exposure, prompting guidelines to avoid valproate in pregnancy due to its dose-dependent causality confirmed in registries.[46] Folate deficiency in early pregnancy may contribute via impaired DNA methylation and one-carbon metabolism essential for orofacial fusion, with low maternal intake associated with modest risk increases (OR ~1.2-1.4 in case-control studies), though meta-analyses of periconceptional supplementation yield mixed preventive effects unlike its robust role in neural tube defects.[47] [48] Evidence from fortification trials shows no consistent reduction in cleft prevalence, suggesting weaker causality.[49] Maternal obesity (BMI ≥30 kg/m²) is linked to higher cleft odds (pooled OR 1.18, 95% CI 1.11-1.26) in meta-analyses, potentially via adipokine dysregulation or inflammation affecting embryonic palate shelf elevation, but adjustment for confounders like diabetes attenuates effects in some cohorts.[50] [51] Alcohol consumption shows inconsistent associations, with ORs ~1.1-1.3 for moderate intake but null in dose-adjusted models, lacking strong causal evidence beyond confounding by smoking.[38] [52] Across factors, relative risks are modest, and population-attributable fractions low, underscoring multifactorial etiology where environmental insults amplify but rarely solely cause disruptions in precise embryonic tissue fusion.Gene-environment interactions
Gene-environment interactions in the etiology of cleft lip with or without cleft palate (CL/P) demonstrate non-additive effects where specific genetic variants heighten susceptibility to environmental exposures, amplifying developmental disruptions during embryogenesis beyond what either factor alone would predict. Empirical studies, including genome-wide analyses of parent-offspring triads, have identified loci such as ESRRG, where maternal periconceptional vitamin use interacts with variants to modify CL/P risk, indicating that nutrient availability can exacerbate or mitigate genetically conferred vulnerabilities in craniofacial morphogenesis. Similarly, variants in RUNX2 show interaction with environmental tobacco smoke, elevating odds ratios for CL/P in exposed carriers compared to non-interaction models. These findings underscore causal mechanisms rooted in impaired cellular signaling and repair pathways, where environmental insults exploit genetic weaknesses rather than independently driving outcomes.[53][54] A prominent example involves polymorphisms in the IRF6 gene, which encodes a transcription factor critical for oral epithelial differentiation and wound healing. Maternal smoking during pregnancy, introducing toxins that impair fetal tissue repair, synergizes with IRF6 variants like rs642961 allele A, yielding elevated odds ratios (e.g., OR=1.74 for combined cleft types) in interaction analyses from case-control studies; this exceeds additive risks, as smoking alone increases CL/P likelihood by approximately 1.3-fold, but genetic carriers face compounded impairment in palate fusion. Peer-reviewed cohort data confirm this synergy, attributing heightened penetrance to disrupted IRF6-mediated responses to oxidative stress from nicotine derivatives. Such interactions highlight how genetic baselines predetermine environmental impact, with heritability estimates for CL/P around 70-80% modulated by these effects.[55][56][57] Recent investigations into translational machinery reveal further GxE dynamics. A 2025 study identified a non-syndromic CL/P risk locus intersecting an enhancer active in embryonic craniofacial tissues, linking variants to tRNA splicing defects that generate aberrant tRNA fragments; these disrupt protein synthesis in neural crest-derived cells, precipitating cleft formation. While primarily genetic, this mechanism implies sensitivity to environmental stressors—such as folate deficiency or toxin-induced proteotoxic stress—that could intensify translation errors during critical gestational windows (e.g., weeks 4-10), as tRNA processing vulnerabilities amplify under metabolic perturbations. Genome-wide GxE scans estimate these interactions explain additional risk variance (up to 10-20% in some models) not captured by marginal effects, emphasizing multifactorial causality over isolated nurture. Public health emphases on modifiable exposures like smoking, while evidence-based for risk reduction in susceptible genotypes, often understate dominant genetic architectures, as twin studies show concordance rates far exceeding environmental attributions alone.[58][59][60]Epidemiology
Global and regional prevalence
Cleft lip and/or cleft palate (CL/P) affects approximately 1.5 per 1,000 live births globally, with combined orofacial cleft prevalence ranging from 1 to 2 per 1,000 births based on aggregated data from birth registries and meta-analyses.[61][62] Isolated cleft palate (CP) occurs at rates of about 0.5 per 1,000, while CL/P combined is around 1 per 1,000.[62] These figures derive from systematic reviews of hospital and population-based records, though underreporting in low-resource settings may underestimate true incidence.[61] Regional disparities show prevalence highest in Asian populations at 1.8 to 3.6 per 1,000 births and among Native American groups, often exceeding 2 per 1,000, compared to lower rates in African populations of 0.5 to 1 per 1,000.[63][64] In Europe, EUROCAT registries report CL/P at 0.9 per 1,000 births (8.98 per 10,000), with total orofacial clefts aligning closer to 1.2 to 1.5 per 1,000 across monitored regions.[65] These variations reflect consistent patterns in multi-ethnic studies, with Asian and indigenous American cohorts showing 2- to 4-fold higher rates than African-derived groups.[63][66] Sex ratios differ by cleft type: CL/P exhibits a 2:1 male-to-female predominance, while isolated CP shows a reverse 1:2 ratio favoring females.[67][68] This dimorphism holds across global datasets, with males comprising about 60% of CL/P cases in population studies.[69]Racial and ethnic disparities
Prevalence rates of orofacial clefts, including cleft lip with or without cleft palate (CL/P) and isolated cleft palate (CP), exhibit marked racial and ethnic disparities in the United States, with empirical data from birth records highlighting biological rather than environmental dominance in explaining variances. Analysis of U.S. natality data from recent years shows the highest rates among Native American/Alaska Native populations at 32.8 per 10,000 live births (95% CI: 30.4–35.2), followed by Asians at 27.5 per 10,000 (95% CI: 26.2–28.8), while Black populations consistently demonstrate the lowest rates, approximately 6–9 per 10,000 depending on subtype and period.[70][71] These patterns align with broader ancestry-based trends, where CL/P incidence reaches 1 in 500 among Asian-descent groups and drops to 1 in 2,500 among those of African descent.[72] Genetic ancestry strongly correlates with these differences, independent of socioeconomic or cultural confounders in crude prevalence estimates. Studies of admixture in South American populations link elevated CL/P susceptibility to Amerindian genetic components, mirroring high rates in Native American groups.[73] Similarly, genome-wide association analyses confirm that orofacial cleft risk alleles vary by continental ancestry, with enrichment in East Asian and Native American lineages contributing to higher penetrance, whereas protective factors predominate in African-ancestry profiles.[72] Longitudinal U.S. trend data from 2010–2021 reinforce that Native American rates exceed white reference groups by 36–44%, persisting across cohorts without attenuation from modifiable risks like maternal smoking or nutrition, underscoring heritable mechanisms over access-related artifacts.[74] Such disparities reflect underlying allelic frequency differences rather than uniform environmental pressures, as evidenced by consistent global patterns tied to migration and admixture histories; for instance, admixed Latin American populations show intermediate rates scaling with indigenous ancestry proportions.[73] Peer-reviewed registries emphasize that while syndromic clefts may introduce minor variations, nonsyndromic forms—comprising over 70% of cases—drive the ethnic gradients through polygenic inheritance.[72] This causal framework prioritizes empirical genetic architecture over speculative equalization narratives.Temporal trends and modifiable risks
In the United States, the prevalence of cleft lip with or without cleft palate (CL/P) exhibited a slight, non-significant decline from 1.65 per 1,000 births in 2001 to 1.17 per 1,000 births in 2021, with an annual percent change of -0.82 (95% CI: -2.18 to 0.56).[75] Globally, orofacial cleft incidence decreased significantly from 1990 to 2021, though low- and middle-socio-demographic index regions retained the highest burden in 2021.[76] Folic acid fortification of food supplies has correlated with modest reductions in orofacial cleft prevalence, with one population-based analysis reporting a prevalence ratio of 0.94 (95% CI: 0.92-0.96) post-fortification compared to pre-fortification periods.[77] Meta-analyses indicate periconceptional folic acid supplementation may lower nonsyndromic oral cleft risk, though evidence remains inconsistent across studies and weaker than for neural tube defects.[78] Maternal smoking represents a key modifiable risk, with meta-analyses estimating a 1.3-fold increased odds of CL/P among exposed offspring; smoke-free legislation in England, Wales, and Northern Ireland was associated with an 8% incidence reduction (95% CI: 1-14%).[79][80] No empirical data supports broad environmental toxins as drivers of rising cleft rates, as observed temporal declines align more closely with public health interventions targeting smoking and nutrition.[81] Maternal obesity, however, elevates cleft risk (OR 1.28, 95% CI: 1.08-1.51), and amid increasing pre-pregnancy obesity prevalence, projections suggest potential upticks in obesity-attributable cases by 2025 without targeted weight management or metabolic interventions.[38][82]Clinical Features
Characteristics of cleft lip
Cleft lip manifests as a visible fissure or gap in the upper lip, resulting from incomplete fusion of the embryonic facial processes, and is classified by laterality and extent. Unilateral cleft lip affects one side, more commonly the left, producing asymmetry in the lip and nasal structures, while bilateral cleft lip involves both sides with a central prolabial segment separated from the lateral lip elements.[83][84]
The severity distinguishes complete clefts, which extend fully from the vermilion border through the lip to the nasal floor, disrupting the continuity of the orbicularis oris muscle and exposing the underlying maxilla, from incomplete clefts, where a fibrous or mucosal bridge known as Simonart's band partially connects the cleft margins, preserving some nasal sill integrity. In unilateral forms, the orbicularis oris muscle exhibits discontinuity, with fibers abnormally inserting into the alar base rather than forming a functional sphincter, leading to lip shortening and nasal deformity characterized by ala flattening and columellar deviation toward the non-cleft side. Bilateral clefts feature symmetrical muscle disruptions on both sides, often with a flattened nasal tip and absent philtral columns.[85][86][83]
Newborns with cleft lip face immediate feeding challenges due to impaired lip seal formation around the nipple, resulting in inefficient sucking, reduced negative intraoral pressure, and occasional nasal milk reflux, though these issues are generally less obstructive than in isolated cleft palate cases.[87][88]
Characteristics of cleft palate
A cleft palate consists of a fissure or gap in the secondary palate, located posterior to the incisive foramen, resulting from failed fusion of the palatal shelves during embryonic development between weeks 6 and 12 of gestation.[1] This defect may involve the soft palate alone, extend anteriorly to include the hard palate, or present as an incomplete or complete cleft, with the uvula, soft palate musculature, and bony structures variably affected.[89] In submucous cleft palate, an intact mucosal covering conceals underlying muscular diastasis and a notched hard palate (bifid uvula or zona pellucida), distinguishing it from overt clefts where the defect is visibly open.[1][90] The soft palate's abnormal insertion of the levator veli palatini muscle disrupts velar elevation, causing velopharyngeal insufficiency (VPI), where the velum fails to seal against the posterior pharyngeal wall during speech and swallowing.[91] This results in hypernasal resonance, nasal air emission, and compensatory articulation errors, as air escapes into the nasal cavity, reducing oral pressure for consonants.[92] Submucous clefts, despite appearing intact superficially, often exhibit this functional deficit due to disorganized muscle fibers, with up to 50% of cases showing speech impairment from VPI.[93] Malformation of the tensor veli palatini muscle, which inserts abnormally in cleft palate, impairs Eustachian tube dilation and ventilation, leading to persistent middle ear effusion and conductive hearing loss.[94] This dysfunction arises from the muscle's deviated path and reduced tension, preventing effective opening of the cartilaginous Eustachian tube portion during swallowing or yawning.[95] Isolated cleft palate, comprising approximately one-third of orofacial clefts, demonstrates female predominance, potentially linked to later palatal shelf closure in females during embryogenesis.[96][97]Associated physical complications
Children with cleft palate exhibit Eustachian tube dysfunction primarily due to aberrant insertion of the tensor veli palatini muscle into the malformed soft palate, impairing middle ear aeration and resulting in recurrent otitis media with effusion (OME) at rates approaching 90%.[98] [99] This chronic condition stems from inadequate clearance of middle ear secretions and negative pressure, fostering bacterial overgrowth and effusion persistence even after palatal repair.[100] The associated conductive hearing loss arises mechanistically from OME-induced ossicular chain impedance, with prevalence estimates ranging from 20% to 30% in cleft palate patients, though some cohorts report up to 50% persistence into adulthood due to unresolved tubal anomalies.[101] [102] Conductive deficits predominate, but mixed or sensorineural components occur at elevated rates compared to the general population, correlating with cumulative otitis exposure.[103] Dental anomalies frequently accompany cleft lip with or without palate, driven by disrupted odontogenesis in the cleft-adjacent alveolar processes; hypodontia affects 28% to 79% of cases, most commonly involving maxillary lateral incisors, while supernumerary teeth, delayed eruption, and morphological irregularities occur in up to 50% of affected dentition.[104] [105] Malocclusion, including Class III skeletal patterns, manifests in over 50% due to asymmetric maxillary growth inhibition from the cleft gap and scar tissue contracture.[106] Midface hypoplasia represents a growth sequela from inherent maxillary segment deficiency in bilateral clefts and postoperative scarring, yielding sagittal retrusion measurable by cephalometric analyses showing reduced maxillary prominence relative to cranial base norms.[107] [108] This underdevelopment causally links to diminished nasomaxillary complex advancement, exacerbating facial disharmony independent of syndromic involvement. Oronasal fistulas, persisting anatomical communications between oral and nasal cavities post-palatoplasty, arise from wound dehiscence or inadequate tissue mobilization, with meta-analytic rates of 4.9% (95% CI: 3.8-6.1%) across primary repairs, higher in complete clefts due to greater tension on closure sites.[109] These defects mechanically enable nasal reflux of oral contents, perpetuating infection risk until secondary correction.[110]Dental and psychosocial impacts
Individuals with cleft lip and/or palate commonly experience dental anomalies, with hypodontia (tooth agenesis) reported in 28-66% of cases, most frequently affecting the maxillary lateral incisors adjacent to the cleft site.[111] Supernumerary teeth occur less often, at rates around 5-6%, while overall, 93% of unilateral cleft lip and palate (UCLP) cases and 96% of bilateral cleft lip and palate (BCLP) cases exhibit at least one anomaly.[105][112] These irregularities arise from disrupted odontogenesis in the cleft region, compounded by alveolar bone defects, often necessitating orthodontic interventions or prosthetics for functional alignment. Class III malocclusion predominates due to maxillary hypoplasia, affecting occlusion and mastication long-term if unaddressed.[113] Psychosocially, children with cleft lip and/or palate face elevated risks of teasing and bullying, approximately twice that of peers without clefts, primarily linked to visible facial differences and speech impediments, which correlate with lower self-esteem and heightened anxiety during school years.[114][115] Longitudinal studies indicate transient dips in self-esteem during adolescence, often tied to unmet expectations around appearance or social integration, yet surgical repairs and multidisciplinary support demonstrably improve social-emotional well-being and satisfaction with facial features.[116] Despite these challenges, resilience is common, with many individuals achieving normative psychosocial adjustment through adaptive coping and family support, underscoring individual variability rather than uniform impairment; factors like cleft visibility or gender show limited predictive power for outcomes.[117][118] Overemphasis on pathology in appearance-related concerns risks pathologizing natural self-consciousness, as empirical data reveal no inherent predisposition to chronic mental health disorders absent external stressors like persistent bullying.[119]Diagnosis
Prenatal detection methods
Prenatal detection of cleft lip and palate primarily relies on fetal ultrasound performed during the second trimester, typically between 18 and 20 weeks of gestation, as part of routine anomaly screening. Two-dimensional (2D) ultrasound can visualize the fetal profile and upper lip, enabling identification of cleft lip with a sensitivity of 75-90% in population-based screening programs.[120] However, detection of isolated cleft palate remains challenging with 2D ultrasound alone, achieving sensitivities as low as 0-1.4% due to difficulties in imaging the secondary palate.[120] Three-dimensional (3D) and four-dimensional (4D) ultrasound techniques enhance diagnostic accuracy by providing multiplanar reconstructions of the fetal face and palate, particularly when cleft lip is suspected. Studies report that 3D ultrasound improves specificity and sensitivity for orofacial clefts, with detection rates reaching 95-100% for cleft lip in enhanced protocols and better visualization of palatal defects compared to 2D alone.[121][122] The combination of 2D and 3D modalities is recommended for confirmatory evaluation, though 3D/4D remains operator-dependent and is not universally available in routine screening.[121] Amniocentesis may be offered following ultrasound detection of a cleft, especially in cases with additional anomalies suggestive of syndromic associations, to perform karyotyping or genetic testing for chromosomal defects. While isolated clefts do not independently elevate chromosomal risk, up to 30% of cleft cases involve syndromes identifiable through amniotic fluid analysis, with procedure-related miscarriage risk below 0.1-0.3%.[123][124] Overall prenatal detection rates for cleft lip and palate vary from 9% to 100% across studies, higher for cleft lip (often 70-90% in optimized settings) and lower for isolated palate-only cases, reflecting advancements in imaging since the 2010s.[125] In high-resource environments with standardized protocols, rates have risen to 30-70% for combined cleft lip/palate by 2020-2024, driven by improved ultrasound resolution.[124] Limitations include operator expertise, fetal position, maternal body mass index, and oligohydramnios, which contribute to false negatives; false positives occur in approximately 1-2% of suspected cases but are minimized with expert review.[126][125] These factors underscore the need for specialized fetal medicine centers for equivocal findings.Postnatal classification systems
Postnatal classification of cleft lip and palate relies on standardized anatomical systems to describe the extent and location of defects, facilitating communication among clinicians, treatment planning, and prognostic assessment. The LAHSHAL system, introduced in 1987, provides a concise, palindrome-based notation for unilateral or bilateral clefts involving the lip (L), alveolus (A), hard palate (H), and soft palate (S), with uppercase letters denoting complete clefts and lowercase for incomplete ones; it assesses structures sequentially from right to left, enabling precise morphological documentation without ambiguity.[127] [128] This system has demonstrated high inter-observer reliability in clinical studies, with agreement rates exceeding 90% after training, supporting its utility in outcome tracking and research.[129] For cleft palate, the Veau classification, established in 1931, categorizes defects into four groups based on anatomical involvement: Class I involves only the soft palate; Class II extends to the posterior hard palate; Class III includes unilateral complete clefts of the lip, alveolus, and palate; and Class IV denotes bilateral complete clefts.[130] This system emphasizes the secondary palate's integrity and laterality, correlating with surgical complexity and functional outcomes such as speech development, as validated in longitudinal studies showing Class III and IV cases requiring more interventions for velopharyngeal insufficiency.[128] Empirical data from cohort analyses confirm its prognostic value, with Class I defects associated with lower rates of postoperative hypernasality compared to Classes III and IV.[131] Functional classifications complement anatomical ones by incorporating assessments like velopharyngeal gap measurement via nasendoscopy or videofluoroscopy, quantifying insufficiency (e.g., gaps >5 mm predicting poor closure post-surgery).[132] These integrate with anatomical systems to guide multidisciplinary decisions, though variability in application underscores the need for standardized protocols. Recent advancements incorporate 3D imaging, such as stereophotogrammetry and cone-beam computed tomography, for volumetric analysis of palatal and alveolar defects, improving classification accuracy over 2D methods by up to 20% in severity grading and enabling personalized prognosis.[133] [134] Studies from 2023 onward report enhanced inter-rater agreement with 3D models, shifting protocols toward dynamic, patient-specific evaluations while retaining core anatomical frameworks like LAHSHAL and Veau.[135]Genetic testing and syndrome identification
Targeted gene panels evaluate known cleft-associated loci, including IRF6 and MSX1, to detect pathogenic variants contributing to both syndromic and nonsyndromic orofacial clefts. Variants in IRF6 underlie Van der Woude syndrome, characterized by cleft lip or palate alongside lip pits, and account for approximately 12% of genetic risk in nonsyndromic cleft lip with or without palate (NSCL/P), tripling recurrence odds in affected families.[136][137] MSX1 mutations link to nonsyndromic clefts often with tooth agenesis, prompting panel inclusion for cases with dental anomalies.[23] These panels, covering 20-50 genes, suit initial testing in familial nonsyndromic cases or mild syndromic features, though diagnostic yields remain low (under 5%) absent strong family history due to the polygenic nature of most NSCL/P.[138][137] In syndromic clefts, where extracraniofacial anomalies suggest monogenic etiology, whole-exome sequencing (WES) identifies causal variants in 10-20% of cases, with curated panels enhancing yield to 15.1% by prioritizing cleft-relevant genes.[139] For cleft palate alone, yields reach 17.6%, dropping to 9% for cleft lip with palate, reflecting variable penetrance and locus heterogeneity.[140] WES proves cost-effective for recurrence counseling in multiplex families, enabling precise risk stratification beyond empirical 3-5% sibling recurrence for isolated NSCL/P.[138] Recent 2024 meta-analyses affirm NSCL/P associations with IRF6 polymorphisms like rs642961 and rs2235371, consolidating evidence across diverse populations for elevated susceptibility under dominant models.[141] These findings support targeted variant screening for familial risk assessment, yet polygenic risk scores aggregating such loci lack clinical utility, as modest per-allele effects (odds ratios <1.5) and environmental confounders preclude reliable prediction outside research contexts.[142] Routine polygenic testing thus awaits validation in prospective cohorts to balance informativeness against false reassurance in low-penetrance scenarios.[143]Treatment Approaches
Multidisciplinary team management
The management of cleft lip and cleft palate necessitates a coordinated multidisciplinary team to integrate surgical, orthodontic, speech, audiological, and supportive interventions, thereby optimizing developmental trajectories over the patient's lifespan. Core team members typically include a craniofacial or plastic surgeon for primary repairs, an orthodontist for dental alignment, a speech-language pathologist for articulation and resonance assessment, and an audiologist for monitoring otitis media and hearing thresholds, often supplemented by an otolaryngologist, geneticist, and nurse coordinator to facilitate family-centered care.[144][145] This structure contrasts with fragmented solo-provider models by enabling protocol-driven evaluations at standardized intervals, such as quarterly clinics in infancy transitioning to annual reviews.[146] Evidence from longitudinal evaluations demonstrates that multidisciplinary cleft teams yield superior coordination compared to isolated specialist care, with integrated follow-ups resulting in more precise therapeutic decisions—averaging 2-3 targeted interventions per annual visit—and reduced delays in addressing complications like velopharyngeal dysfunction.[147] For instance, team-managed cohorts exhibit lower rates of secondary surgical revisions, attributed to proactive orthodontic and speech monitoring that preempts maxillary hypoplasia or hypernasality, though isolated cleft lip cases may require less intensive long-term oversight.[148] Standard timelines prioritize lip repair between 3 and 6 months to support feeding and facial aesthetics, followed by palate closure at 9 to 12 months to align with speech emergence, ensuring the infant's weight exceeds 5 kg and hemoglobin levels are adequate for anesthesia safety.[149][150] Recent evidence from randomized controlled trials, including a 2023 multicenter study, indicates benefits from advancing palate repair to 6 months in otherwise healthy infants, correlating with a 39% relative reduction in velopharyngeal insufficiency at age 5 without compromising midfacial growth.[151] These protocols are evidence-based, drawing from centers achieving high-volume expertise (e.g., >50 cases annually per team) to minimize variability.[152]Surgical repair of cleft lip
The primary surgical repair of cleft lip is generally performed between 3 and 6 months of age, balancing the need for early anatomical closure to support feeding, facial development, and psychosocial benefits against risks of prematurity in neonatal intervention.[153] [154] This timing aligns with criteria such as the "rule of 10s" originally proposed by Millard—infant age around 10 weeks, weight of 10 pounds, and hemoglobin level of 10 g/dL—to minimize anesthesia-related complications while enabling nasal floor and alveolar alignment during repair.[155] The Millard rotation-advancement technique, introduced in 1955, remains the predominant method for unilateral cleft lip repair, prioritizing minimal tissue excision to achieve anatomical fidelity in lip height, vermilion alignment, and muscular orbicularis oris continuity.[156] [157] The procedure involves a medial backcut incision along the non-cleft philtral column to rotate the Cupid's bow peak downward, compensating for vertical deficiency, while a lateral advancement flap from the cleft side fills the resulting gap; a small backcut on the lateral element ensures tension-free closure and white roll continuity.[158] Concomitant repairs include reapproximation of the nasal floor to prevent oronasal fistula and alignment of the underlying alveolus for future dental arch integrity, with muscle plication restoring dynamic lip function.[159] For bilateral cases, symmetric advancement flaps are adapted to centralize the prolabial segment.[160] Pre-surgical nasoalveolar molding (NAM), initiated shortly after birth, is frequently integrated to precondition tissues by gradually reducing cleft width, repositioning the displaced alveolus, and reshaping the nasal cartilage for enhanced intraoperative symmetry.[161] [162] Clinical studies demonstrate NAM efficacy in decreasing the cleft gap by up to 50-70% and improving columellar length, though long-term superiority over surgery alone remains debated due to limited randomized evidence.[163] Postoperative complications include hypertrophic scarring, occurring in 8-47% of repairs depending on ethnicity, wound tension, and genetic factors, often manifesting within 3-6 months and requiring interventions like silicone sheeting or laser therapy.[164] [165] Other risks encompass wound dehiscence (up to 14%) and minor fistulas, with overall rates influenced by surgical precision and adjunctive scar management.[166]Surgical repair of cleft palate
Surgical repair of the cleft palate primarily seeks to close the oronasal communication, reposition palatal muscles for improved velopharyngeal function, and minimize complications such as fistulas, thereby supporting speech development and Eustachian tube function.[167] The procedure typically involves dissection and realignment of the levator veli palatini muscles, which are abnormally oriented in the cleft, to form a functional sling.[168] Among techniques, the Furlow palatoplasty, employing double-opposing Z-plasty on both oral and nasal layers, has demonstrated advantages over conventional two-flap palatoplasty (e.g., von Langenbeck) in achieving velopharyngeal competence. This method lengthens the soft palate and reorients muscles without pushback, resulting in lower rates of hypernasality and reduced need for secondary speech surgery in long-term follow-up.[169] [170] A 2012 comparative study found Furlow superior for perfect velopharyngeal closure, with hypernasality scores significantly better than two-flap repairs.[169] Debates persist on one-flap versus two-flap variants, but evidence from randomized assessments favors Z-plasty for speech normalization, with success rates exceeding 80% in avoiding compensatory articulation disorders.31099-1/fulltext) [171] Timing of repair has shifted toward earlier intervention, often 6-9 months, based on cohort data showing reduced velopharyngeal insufficiency compared to delays beyond 12 months.[172] A 2023 randomized trial indicated that 6-month repair lowered VPI risk, though some analyses note potential for more secondary procedures; however, 2025 preprints on delayed repairs affirm early closure's benefits for functional outcomes without disproportionate growth deficits.[173] Primary closure occurs under general anesthesia, with multilayer suturing to ensure tension-free approximation and fistula prevention.[174] Oronasal fistulas, abnormal communications persisting post-repair, arise in 5-15% of cases, influenced by cleft severity, surgeon experience, and technique.[175] [110] Incidence varies widely (up to 60% in high-risk cohorts), but Furlow and two-flap methods with acellular dermal matrices reduce rates to under 10% by enhancing vascularity and closure integrity.[176] [177] While palatoplasty scarring can constrain midfacial advancement, evidence critiques exaggerated concerns, as the cleft defect itself promotes maxillary retrusion; studies on modified Furlow show no significant long-term growth detriment beyond inherent hypoplasia, prioritizing speech gains.[178] [171] Delayed hard palate closure variants mitigate impacts but risk speech delays, underscoring trade-offs resolved via multidisciplinary timing.[179]Adjunctive therapies for speech and hearing
Children with cleft palate are prone to recurrent otitis media with effusion (OME) due to Eustachian tube dysfunction, resulting in conductive hearing loss that affects up to 100% of cases without intervention.[180] Tympanostomy tube placement, often performed early and as standard care in many protocols, significantly improves hearing thresholds and reduces effusion persistence, with evidence from cohort studies showing sustained benefits when tubes are inserted at the time of palate repair.[181] Repeated insertions are common, particularly in syndromic cases, where rates exceed 85%.[182] While randomized trials in general pediatric populations demonstrate tubes' role in lowering acute otitis episodes compared to medical management alone, their application in cleft cohorts emphasizes auditory support to mitigate developmental delays.[183] Post-primary palate repair, residual velopharyngeal insufficiency (VPI) contributes to hypernasal speech in 28-40% of children aged 5-15 years.[184] Speech-language therapy, typically beginning after age 2 once surgical healing stabilizes, focuses on articulation training and resonance control to address compensatory misarticulations and nasal emission. Intensive programs, including those enhancing oral-nasal balance via prosthetic aids like speech bulbs, provide preliminary evidence of reduced hypernasality, though nonspeech oral motor exercises show no efficacy for velopharyngeal improvement or sound remediation.[185][186] For persistent severe VPI unresponsive to therapy, adjunctive pharyngeal flap surgery achieves velopharyngeal competence in the majority of cases, with randomized controlled trials reporting equivalent short-term speech outcomes to sphincter pharyngoplasty, including normalized resonance in over 70% at one year postoperatively.[187] Revision rates hover around 20%, comparable across techniques when patient selection accounts for anatomy and function.[188] Randomized trials of early speech interventions, such as parent-implemented naturalistic approaches before or shortly after palate repair, yield improved consonant production and lexical growth in toddlers, underscoring benefits over delayed or no therapy for mitigating long-term deficits.[189][190] These adjunctive strategies integrate multidisciplinary monitoring to optimize communication outcomes, with ongoing trials evaluating intensive versus standard therapy timing.[191]Feeding and orthodontic interventions
Infants with cleft lip and/or palate experience feeding difficulties primarily due to impaired ability to generate negative pressure for suction, leading to inefficient milk transfer and risk of aspiration or nasal regurgitation.[192] Specialized feeding bottles, such as the Haberman feeder or Mead Johnson Cleft Nurser, address this by employing compressible reservoirs and valves that allow controlled flow via parental compression rather than infant suction, improving intake efficiency.[193] A systematic review of interventions found specialty bottles utilized in 21% of cases, correlating with better weight gain compared to standard bottles.[192] Breastfeeding remains challenging but feasible with techniques like semi-upright positioning, frequent small feeds, and supplemental pumping to maintain supply, as supported by clinical guidelines emphasizing breast milk benefits despite anatomical barriers.[194] Orthodontic interventions begin early to guide maxillary segment alignment and prevent skeletal discrepancies. Presurgical nasoalveolar molding appliances, applied shortly after birth, reposition displaced segments prior to lip repair, facilitating better surgical outcomes and arch form.[195] Post-primary surgery, rapid maxillary expansion using palatal expanders addresses transverse deficiencies common in cleft cases, typically initiated around ages 8-10 years before alveolar bone grafting.[196] Secondary alveolar bone grafting, performed between 8 and 12 years—ideally prior to permanent canine eruption—fills the cleft defect with autologous iliac crest bone, stabilizing the alveolus and enabling orthodontic tooth movement, with reported success rates of 91% at long-term follow-up based on radiographic bone fill and dental outcomes.[197] Comprehensive fixed orthodontic therapy follows, achieving proper alignment and occlusion in approximately 80-90% of cases when sequenced with grafting and surgery, thereby mitigating malocclusion risks.[198] Long-term monitoring ensures retention appliances prevent relapse, with multidisciplinary timing critical for optimal skeletal and dental harmony.[195]Prognosis and Outcomes
Short-term surgical results
Short-term surgical results for cleft lip repair typically demonstrate high primary success rates, with wound healing achieving approximately 95% success and complication rates, including infection and dehiscence, remaining below 5% in contemporary series.[199] [200] For cleft palate repair, complication rates are higher, often around 15-16%, primarily due to wound breakdown and early fistulas, though modern protocols like surgical safety checklists have reduced infections, dehiscence, and fistulas significantly.[199] [201] Nasoalveolar molding (NAM) and presurgical orthopedics improve immediate postoperative alignment, with digital and AI-assisted techniques emerging since 2023 enhancing precision in segment approximation and nasal symmetry.[202] [203] Symmetry scores post-lip repair, assessed via anthropometric measures, show good outcomes in over 67% of cases, while oronasal fistula absence serves as a key short-term metric for palate repair, with rates as low as 3.1% in optimized settings.[166] [204] These metrics underscore the efficacy of standardized techniques in minimizing early revisions and ensuring stable wound closure within weeks postoperatively.[205]Long-term functional and aesthetic outcomes
Longitudinal cohort studies of patients with repaired cleft lip and palate demonstrate that functional outcomes in adulthood frequently approach normalcy for speech, mastication, and nasal airflow, though persistent challenges such as hypernasality or velopharyngeal insufficiency affect 10-30% of cases, often necessitating secondary surgeries like pharyngoplasty in 15-25% of unilateral cleft lip and palate (UCLP) patients.[206][207] With intensive speech therapy, long-term intelligibility reaches 80-95% in motivated cohorts, particularly those undergoing early palate repair and velar muscle repositioning, as evidenced by follow-up data into the third decade of life showing sustained improvement even after delayed hard palate closure.[208][209] Dental function post-alveolar bone grafting yields high success, with 91% of grafts supporting canine eruption and orthodontic alignment by adolescence, enabling functional occlusion in most patients despite initial maxillary hypoplasia.[197][210] Aesthetic outcomes vary by cleft extent and revision history, with lip symmetry satisfaction reported at 70-95% among young adults, though nasal deformities persist as the primary concern, prompting secondary rhinoplasty in 35-74% of cases due to asymmetric tip projection and columellar deficiency.[211][212] In bilateral cleft lip and palate (BCLP), midfacial growth disturbances are more pronounced, leading to Class III malocclusion in up to 50% without orthognathic intervention, whereas UCLP patients exhibit better transverse maxillary development and lower revision rates for scar revision (20-40%).[213][214] Patient-reported quality of life metrics, including self-esteem and social integration, align closely with general population norms by adulthood in 70-85% of treated individuals, contingent on multidisciplinary follow-up, though bilateral cases show higher rates of dissatisfaction (up to 40%) linked to iterative procedures.[215][216]This image illustrates a long-term aesthetic result following primary cleft lip repair, with minimal visible scarring by early childhood.
Factors influencing success rates
The timing of primary surgical intervention significantly influences long-term outcomes in cleft palate repair, with empirical evidence indicating superior speech proficiency, reduced hearing loss, and improved dentofacial growth when performed at 6 months of age compared to 12 months.[151] This causal link arises from the critical window for palatal muscle development and Eustachian tube function maturation, where earlier closure minimizes compensatory speech patterns and maxillary hypoplasia.[217] Delays beyond 12 months correlate with increased articulation errors and secondary interventions in up to 18% of cases. Presence or absence of associated genetic syndromes represents a primary determinant of surgical success, as syndromic clefts (e.g., those linked to Pierre Robin sequence or 22q11 deletion) necessitate altered protocols and exhibit higher perioperative complication rates, including prolonged intubation needs and fistula formation exceeding non-syndromic baselines by factors of 2-3.[219] Non-syndromic isolated clefts, comprising approximately 70% of cases, achieve revision rates 40-50% lower due to fewer anatomical anomalies and better tissue pliability.[220] Genetic profiling prior to surgery enables risk stratification, with syndromic patients facing elevated mortality risks up to 52% in comorbid scenarios versus under 6% otherwise.[221] Socioeconomic factors exert a downstream effect on outcomes through barriers to timely multidisciplinary follow-up, with children from lower-income quartiles experiencing palate repairs delayed by 2-4 months on average, correlating with diminished language development and higher velopharyngeal insufficiency rates.[222] Public insurance and non-urban residence amplify disparities, reducing adherence to adjunctive therapies like speech pathology by 20-30% and elevating suboptimal aesthetic revisions.[223] Recent 2024 analyses confirm these gradients persist despite protocol standardization, underscoring access as a modifiable causal barrier independent of biological severity.[224] Adherence to postoperative protocols, including nutritional support and orthodontic compliance, further modulates success, with non-compliance doubling secondary surgery needs via exacerbated scar contracture and malocclusion.[225] Maternal smoking, while primarily etiologic, indirectly worsens repair efficacy through impaired wound healing and heightened infection risk in exposed neonates, though direct revision multipliers remain underquantified in cleft-specific cohorts.[226] Despite optimal interventions, 10-20% of patients manifest persistent hypernasality or articulation deficits by age 5, necessitating pharyngoplasty, as velopharyngeal closure adequacy varies inherently with palatal musculature even post-early repair.[227][228]Societal and Ethical Dimensions
Cultural perceptions and stigma
In many non-Western societies, cleft lip and palate (CL/P) have historically been attributed to supernatural causes such as witchcraft, sorcery, ancestral displeasure, or divine retribution, fostering significant stigma and social isolation for affected individuals and their families. For instance, a study in Zimbabwe involving parents of children with CL/P found that 38 attributed the condition to witchcraft, with 19% of mothers reporting divorce shortly after birth, reflecting community rejection and familial breakdown.[229] Similarly, among South African traditional healers, clefts are commonly linked to spirits or witchcraft, leading to treatments involving plant and animal products rather than surgical intervention, which delays access to effective care.[230] These beliefs persist in low-resource African contexts, where qualitative research in Kenya revealed parents experiencing profound social and psychological distress from stigma communication, including accusations of moral failing or curses, often resulting in concealment of the child and avoidance of public spaces.[231] Such causal attributions empirically correlate with reduced healthcare-seeking behavior, as families prioritize ritualistic remedies over evidence-based repairs.[232] Cross-cultural surveys highlight variability; for example, pre-Hispanic Mesoamerican artifacts, such as Moche pottery from Peru (circa 100-500 AD), depict individuals with unrepaired clefts, suggesting recognition without uniform stigmatization, though integrated into ritual or symbolic contexts.[233] In contrast, contemporary non-Western views in regions like parts of Asia and Africa continue to frame CL/P as karmic retribution or infection from taboo behaviors, exacerbating discrimination and limiting rehabilitation.[234] These perceptions, rooted in pre-scientific causal reasoning, hinder empirical understanding of CL/P as a multifactorial developmental anomaly amenable to surgical correction, perpetuating cycles of exclusion. In Western societies, medicalization and routine repairs have diminished overt stigma, yet subtle discrimination endures, particularly through parental reports of social inequalities and media underrepresentation. A 2016 study of families with CL/P documented experiences of exclusion from social events and workplace bias against caregivers, with qualitative data from 2020 underscoring ongoing emotional burdens like anxiety over public scrutiny.[235][231] High-profile cases, such as actor Joaquin Phoenix, who was born with a cleft lip repaired in infancy leaving a visible scar, illustrate resilience amid potential stigma; Phoenix has publicly discussed the condition's impact on his self-perception without framing it as defining victimhood, emphasizing treatability and personal agency. While animated media occasionally portrays facial differences, including cleft-like features, analyses show inconsistent narratives that may reinforce rarity over normalcy, though social media increasingly counters this by amplifying patient stories to normalize outcomes.[236] Over-sensitivity to visible differences in Western discourse risks overlooking CL/P's high success rates with intervention (over 90% functional improvement post-repair), potentially amplifying perceived stigma beyond empirical disadvantage.[237]Ethical dilemmas in severe cases
In infants with cleft lip and palate comorbid with trisomy 13 or 18, ethical dilemmas arise primarily from the tension between potential short-term quality-of-life improvements and the underlying high mortality rates of these syndromes. Trisomy 13 carries an 87% first-year mortality rate, while trisomy 18 has an 88% rate, with only 5-15% of affected infants surviving to their first birthday despite supportive care.[238][239] Surgical repair may facilitate feeding and social interaction but offers no causal impact on the lethal chromosomal anomalies, raising questions of medical futility where interventions risk complications like anesthesia-related instability without extending viable lifespan.[240] Surgeons must navigate conflicts between perceived futility and parental demands for repair, as documented in 2023 analyses emphasizing individualized assessment over blanket denial based on diagnosis alone. In cases where comorbidities are stabilized, repairs have succeeded without complications, supporting arguments for intervention to honor autonomy and provide palliation.[241] However, utilitarian perspectives prioritize resource allocation toward infants with isolated clefts or milder syndromes, where long-term functional gains justify surgical risks and costs, given evidence that profound comorbidities amplify perioperative morbidity without proportional benefits.[240] Proponents of persistent intervention, often aligned with respect for life principles, advocate repairing visible defects to affirm infant dignity and family bonding, even in terminal scenarios.[242] Conversely, causal realists and resource ethicists contend that routine repairs in such cases divert finite operative time, beds, and expertise from prognostically favorable patients, as short survival limits enduring utility and heightens overall system strain.[243] These debates underscore the need for multidisciplinary ethics consultations to weigh empirical prognosis against subjective valuations of comfort.[240]Prenatal diagnosis and selective termination debates
Prenatal diagnosis of cleft lip and palate, often via ultrasound at 18-20 weeks gestation, has facilitated selective termination of affected pregnancies in varying rates across jurisdictions, with studies reporting termination incidences ranging from 0% to 92% for isolated clefts, influenced by counseling, cultural norms, and access to services.[244] In specific cohorts, such as one Israeli study, 93% (14 of 15) of diagnosed cases resulted in voluntary termination, while a Hong Kong series post-multidisciplinary counseling showed a 14.5% rate.[245] [246] These figures reflect parental decisions prioritizing perceived quality of life concerns, though cleft conditions are typically non-lethal and surgically correctable with favorable long-term outcomes, raising questions about the proportionality of such choices compared to more impairing anomalies.[247] The practice sparks debates between advocates of parental autonomy—who argue that informed choice allows families to avoid anticipated medical, financial, and emotional burdens—and disability rights proponents who contend it constitutes a form of "soft eugenics" by systematically eliminating fetuses with non-fatal traits, thereby devaluing lives of those with disabilities and pressuring societal norms toward perfection.[248] [249] Critics, including pro-life ethicists, highlight eugenic parallels to historical programs, noting that widespread screening reduces cleft incidence not through prevention but selection, as seen in near-elimination of certain anomalies via termination in places like Iceland for Down syndrome (analogous dynamics apply to treatable defects), without evidence of net societal gains in health or resource allocation.[250] [251] Ethical analyses emphasize cultural variances, with higher termination rates in regions like China for facial deformities, but argue that routinized screening risks commodifying fetal viability based on treatability rather than intrinsic value.[252] [244] Empirically, no rigorous studies demonstrate broad societal benefits from selective terminations for clefts, such as reduced healthcare costs or improved population welfare, as affected individuals often achieve functional independence post-intervention; alternatives like enhanced prenatal support and postnatal care are posited to better uphold causal realism by addressing needs without elimination.[253] Pro-life perspectives, drawing from first-principles valuation of human life irrespective of defect, advocate redirecting resources to family assistance over termination, critiquing mainstream bioethics discourse—often shaped by academic institutions with documented ideological biases—for underemphasizing these eugenic undertones in favor of autonomy narratives.[254] This tension underscores broader ethical dilemmas, where screening's technical advances enable choices that may inadvertently erode diversity and reinforce ableist priorities without proven causal advantages.[255]Access to care and policy implications
Access to comprehensive care for cleft lip and palate remains uneven, particularly in low-income and rural populations where barriers such as geographic distance, limited specialist availability, and financial constraints delay interventions. In the United States, children with public insurance or from rural areas face longer times to surgical appointments, with cost and location cited as primary obstacles, leading to postponed repairs that correlate with heightened risks of complications including prolonged hospital stays and suboptimal speech development. Globally, low- and middle-income countries exhibit stark disparities, with untreated cases prevalent due to inadequate infrastructure, resulting in higher rates of secondary issues like malnutrition and infection when repairs are deferred beyond infancy.[256][257][258] In the US, state-level mandates have expanded coverage, requiring most employer-sponsored and group health plans to include treatments for cleft lip and palate, encompassing surgical, dental, and speech therapies without age limits in many jurisdictions. By 2017, only a minority of states lacked such requirements, reducing out-of-pocket burdens for affected families, though gaps persist in Medicaid reimbursement rates compared to commercial payers, potentially influencing provider participation. These policies aim to mitigate delays, as evidence indicates that repairs performed between 3 and 6 months yield fewer adverse outcomes than later timings, with non-White and lower-socioeconomic groups disproportionately experiencing postponements that elevate complication risks.[259][260][261] Internationally, initiatives by nongovernmental organizations like Operation Smile and Smile Train have facilitated millions of repairs in resource-limited settings, often outperforming public systems strained by wait times exceeding months for elective procedures. In contrast, private facilities consistently demonstrate shorter queues—median waits of under 2 months versus longer public sector delays—correlating with improved functional results, as seen in medical tourism destinations bypassing overburdened national health services. World Health Organization advocacy for global networks has spurred training but yielded variable implementation, with empirical outcomes favoring decentralized, market-driven models that incentivize local capacity over centralized aid dependency.[262][263][264] Policy implications underscore the role of regulatory frameworks in cost dynamics, where undervaluation of cleft procedures in reimbursement schedules discourages specialization, while excessive oversight in public systems inflates administrative burdens without commensurate quality gains. Evidence from economic modeling suggests that easing barriers to private innovation—such as streamlined licensing for multidisciplinary teams—could lower lifetime care expenses, estimated at $65,000 to $100,000 per patient, by promoting efficient, competition-driven delivery over rigid mandates that entrench disparities. Prioritizing incentives for scalable technologies and workforce expansion in privatized contexts aligns with data showing superior access and reduced complication profiles therein.[265][266][267]Research Frontiers
Recent genetic discoveries
In April 2025, researchers at MIT identified a mechanism linking defects in transfer RNA (tRNA) splicing to the development of nonsyndromic orofacial clefts, including cleft lip and palate. The study revealed that variants in a risk locus disrupt tRNA processing, leading to translation errors in craniofacial cells during embryonic development, thereby impairing facial structure formation. This finding underscores the role of post-transcriptional regulation in cleft etiology, challenging models that overemphasize environmental factors alone by demonstrating how genetic disruptions in protein synthesis directly cause these malformations.[268][58] A multi-ancestry genome-wide association study (GWAS) meta-analysis published in December 2024 expanded the known genetic architecture of nonsyndromic orofacial clefts (NSOC), identifying 50 loci associated with cleft lip with or without cleft palate (NSCL/P), including 11 novel loci such as CALD1, SHH, NRG1, and LINC00320. These loci implicate pathways in cell signaling and tissue morphogenesis, with four overlapping risks for both NSOC and NSCL/P subtypes. Building on prior GWAS efforts, this work refines polygenic risk scores (PRS) for NSCL/P prediction, enhancing their accuracy through integration of multi-ethnic data and rare variants, which collectively explain a substantial portion of heritability and refute environment-only causal narratives by quantifying genetic contributions exceeding 20-30% in population variance.[36] Further, a September 2025 analysis identified de novo PRKCI variants in seven individuals with syndromic cleft lip or palate, including Van der Woude syndrome, highlighting rare coding mutations in protein kinase pathways that disrupt epithelial integrity during palate fusion. Complementing these, October 2025 sequencing efforts uncovered novel rare variants in genes regulating craniofacial development, offering causal insights into both syndromic and nonsyndromic forms.[269][270] Translational advances include a September 2025 demonstration of genetic repair in mouse models of cleft lip, where targeted editing restored normal lip morphology in embryos engineered with cleft-inducing mutations, validating CRISPR-based interventions on loci like MSX1 and paving the way for prenatal therapies. These genetic proofs-of-concept emphasize heritability's primacy, with PRS refinements enabling risk stratification that outperforms single-gene models and supports causal genetic determinism over multifactorial ambiguity.[271]Advances in surgical and AI-assisted techniques
Recent studies have demonstrated benefits from optimizing the timing of cleft palate repair, with hard palate closure performed between 13 and 18 months associated with improved maxillary advancement, as measured by greater SNA angles compared to earlier or later timings.[272] A 2025 analysis of treatment cohorts reported reduced time to palate repair in the range of 9-18 months, correlating with enhanced overall healthcare outcomes in unilateral cleft lip and palate cases, though long-term speech benefits require further validation against traditional protocols.[273] These findings build on a 2023 randomized trial showing that primary surgery at 6 months yielded superior speech, hearing, and dentofacial growth outcomes over 12 months, prompting shifts toward earlier interventions within safe developmental windows to minimize velopharyngeal insufficiency.[151] Innovations in minimally invasive techniques have focused on reducing oronasal fistulas, a common complication with rates historically exceeding 10%. A 2025 anatomic approach during unilateral cleft lip and palate repair emphasizes precise dissection at the palato-velar junction, achieving fistula rates below 5% by preserving vascular integrity and minimizing tension, as evidenced in prospective series.[274] Endoscopic "parachute" methods for recurrent fistulas enable multilayer closure with reduced tissue trauma, reporting closure success in over 90% of cases without donor site morbidity.[275] Three-dimensional (3D) printing has enhanced surgical precision through patient-specific guides and models, facilitating accurate maxillary distraction and alveolar grafting in cleft patients. A 2025 review highlighted 3D-printed appliances for preoperative orthopedics, improving cleft width reduction by up to 40% prior to lip repair via customized passive plates derived from intraoral scans.[276] These guides demonstrate superior accuracy in osteotomy placement, with deviations under 1 mm in simulated and clinical applications, leading to better symmetry scores postoperatively.[277] AI integration in presurgical planning has advanced digital workflows, with machine learning algorithms automating cleft size prediction and orthotic design from smartphone scans, reducing planning time by 50% in pilot studies.[278] An ongoing observational trial (NCT06970158) evaluates AI-generated passive plates for newborns, aiming to quantify reductions in cleft gap prior to surgery, with preliminary data suggesting enhanced nasal symmetry.[279] Systematic reviews from 2025 indicate AI-assisted simulations improve surgical rehearsal, yielding 15-20% better speech articulation and facial symmetry in treated cohorts versus non-AI groups, attributed to predictive modeling of tissue dynamics.[280]Animal models and translational insights
Mouse models, particularly genetic knockouts, have been instrumental in elucidating the genetic mechanisms underlying orofacial clefting. For instance, Irf6-null mice exhibit cleft palate accompanied by oral epithelial adhesions and disrupted periderm integrity, mirroring aspects of human syndromic and non-syndromic cleft lip with or without palate (CL/P).[281] These models demonstrate that IRF6 regulates epithelial proliferation and differentiation, with conditional knockouts in neural crest or periderm cells leading to failed palatal shelf fusion due to impaired cell migration and adhesion.[282] Similarly, disruptions in pathways like Hedgehog signaling in mouse embryos result in cleft palate through antagonism of inductive signals critical for facial patterning.[283] Zebrafish models complement mammalian studies by enabling high-throughput visualization of palate shelf dynamics. Morpholino knockdown or CRISPR/Cas9 editing of genes such as irf6 produces orofacial cleft phenotypes, revealing roles in epithelial-mesenchymal interactions and neural crest cell contributions to early palatogenesis.[284] These aquatic models facilitate real-time imaging of shelf elevation and fusion processes, which are evolutionarily conserved across vertebrates, providing mechanistic insights into defects arising from delayed shelf growth or tongue interference.[285] Evolutionary conservation of developmental pathways, including those involving IRF6 and downstream regulators like ESRP1/2, underscores translational potential from animal models to human cleft etiology. Toxin-exposure paradigms, such as chemical-induced models in zebrafish, highlight gene-environment interactions (GxE) by demonstrating how environmental stressors modulate Wnt or methylation pathways to induce clefts, offering parallels to human risk factors like maternal smoking or folate deficiency.[286] These findings have informed candidate gene prioritization in human genome-wide association studies.[287] Despite these advances, animal models face limitations in direct applicability to humans due to species-specific differences in palatal fusion timing, oral cavity morphology, and secondary palate development. For example, mice lack a true equivalent to human primary palate fusion, complicating extrapolation of lip cleft mechanisms, while zebrafish emphasize early ethmoid plate formation over mammalian secondary palate shelves.[288] Nonetheless, these models remain valuable for preclinical testing of therapeutic interventions, such as gene editing or small-molecule modulators of epithelial adhesion, prior to human trials.[289]References
- https://www.[medrxiv](/page/MedRxiv).org/content/10.1101/2025.02.28.25323080v1.full-text