

Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Thigh
View on WikipediaThis article needs additional citations for verification. (April 2011) |
| Thigh | |
|---|---|
 A woman's thighs | |
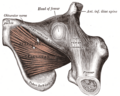
 Cross-section of the thigh showing muscles and bone (latin terminology) | |
| Details | |
| Identifiers | |
| Latin | femur |
| MeSH | D013848 |
| TA98 | A01.1.00.035 |
| TA2 | 160 |
| FMA | 24967 |
| Anatomical terminology | |
In anatomy, the thigh is the area between the hip (pelvis) and the knee. Anatomically, it is part of the lower limb.[1]
The single bone in the thigh is called the femur. This bone is very thick and strong (due to the high proportion of bone tissue), and forms a ball and socket joint at the hip, and a modified hinge joint at the knee.[2]
Structure
[edit]Bones
[edit]The femur is the only bone in the thigh and serves as an attachment site for all thigh muscles. The head of the femur articulates with the acetabulum in the pelvic bone forming the hip joint, while the distal part of the femur articulates with the tibia and patella forming the knee. By most measures, the femur is the strongest and longest bone in the body.[3]
The femur is categorised as a long bone and comprises a diaphysis, the shaft (or body) and two epiphyses, the lower extremity and the upper extremity of femur, that articulate with adjacent bones in the hip and knee.[4]
Muscular compartments
[edit]In cross-section, the thigh is divided up into three separate compartments, divided by fascia, each containing muscles. These compartments use the femur as an axis and are separated by tough connective tissue membranes (or septa). Each of these compartments has its own blood and nerve supply, and contains a different group of muscles.
- Medial fascial compartment of thigh, adductor
- Posterior fascial compartment of thigh, flexion, hamstring
- Anterior fascial compartment of thigh, extension
Anterior compartment muscles of the thigh include sartorius, and the four muscles that comprise the quadriceps muscles – rectus femoris, vastus medialis, vastus intermedius and vastus lateralis.
Posterior compartment muscles of the thigh are the hamstring muscles, which include semimembranosus, semitendinosus, and biceps femoris.
Medial compartment muscles are pectineus, adductor magnus, adductor longus and adductor brevis, and also gracilis.
Because the major muscles of the thigh are the largest muscles of the body, resistance exercises (strength training) of them stimulate blood flow more than any other localized activity.[5]
Blood supply
[edit]
The arterial supply is by the femoral artery and the obturator artery. The lymphatic drainage closely follows the arterial supply and drains to the lumbar lymphatic trunks on the corresponding side, which in turn drains to the cisterna chyli.
The deep venous system of the thigh consists of the femoral vein, common femoral vein, deep femoral vein, the proximal part of the popliteal vein, and various smaller vessels; these are the site of proximal deep vein thrombosis. The perforating veins connect the deep and the superficial system, which consists of the small and great saphenous veins (the site of varicose veins).[7]
Clinical significance
[edit]Thigh weakness can result in a positive Gowers' sign on physical examination.[8]
Thigh injury resulting from sports, whether acute or from overuse, can mean significant incapacity to perform. Soft tissue injury can encompass sprains, strains, bruising and tendinitis.
Runner's knee (patellofemoral pain) is a direct consequence of the kneecap rubbing against the end of the thigh bone (femur). Tight hamstrings and weak thigh muscles, required to stabilize the knee, increase the risk of developing of runner's knee.[9]
Society and culture
[edit]
Western societies generally tolerate clothing that displays thighs, such as short shorts and miniskirts. Beachwear and many athleisure styles often display thighs as well. Professional dress codes may require covering up bare thighs.
Many Islamic countries disapprove of or prohibit the display of thighs, especially by women.
Strategic covering or display of thighs is used in popular fashion around the world, such as thigh-high boots and zettai ryoiki.
Additional images
[edit]-
 Front of thigh muscles from Gray's Anatomy of the human body from 1918.
Front of thigh muscles from Gray's Anatomy of the human body from 1918. -
 Back thigh muscles of the gluteal and posterior femoral regions from Gray's Anatomy of the human body from 1918.
Back thigh muscles of the gluteal and posterior femoral regions from Gray's Anatomy of the human body from 1918. -
 Also showing major blood vessels and nerves.
Also showing major blood vessels and nerves. -
 Cross-section through the middle of the thigh.
Cross-section through the middle of the thigh. -



References
[edit]- ^ "thigh" at Dorland's Medical Dictionary[dead link]
- ^ "Thigh". Cambridge Dictionary. Retrieved 2021-06-23.
- ^ "Facts About Bones in Your Skeleton". Hospital for Special Surgery.
- ^ Bojsen-Møller, Finn; Simonsen, Erik B.; Tranum-Jensen, Jørgen (2001). Bevægeapparatets anatomi [Anatomy of the Locomotive Apparatus] (in Danish) (12th ed.). pp. 239–241. ISBN 978-87-628-0307-7.
- ^ Cespedes, Andrea. "How Important Are Leg Workouts for Muscle Gain?".
- ^ Amarnath C and Hemant Patel (2023). Comprehensive Textbook of Clinical Radiology – Volume III: Chest and Cardiovascular system. Elsevier Health Sciences. p. 1072. ISBN 9788131263617.
- ^ "Thigh". The Lecturio Medical Concept Library. Retrieved 2021-06-23.
- ^ Chang, Richard F.; Mubarak, Scott J. (2011-12-28). "Pathomechanics of Gowers' Sign: A Video Analysis of a Spectrum of Gowers' Maneuvers". Clinical Orthopaedics and Related Research. 470 (7): 1987–1991. doi:10.1007/s11999-011-2210-6. PMC 3369091. PMID 22203329.
- ^ "Medically Sound: Field, Court, and Course Related Injuries – Sports Injuries". Medically Sound. 2020-08-31. Retrieved 2020-11-01.
| International | |
|---|---|
| Other | |
Thigh
View on GrokipediaAnatomy
Bones and joints
The thigh is primarily supported by the femur, the longest, heaviest, and strongest bone in the human body, measuring approximately 26% of an individual's stature on average.[6] The femur consists of a proximal end featuring a spherical head that articulates with the acetabulum, a neck angled at about 125 degrees in adults, and greater and lesser trochanters for muscle attachments; a central cylindrical shaft composed of compact bone externally and trabecular bone internally; and a distal end with medial and lateral condyles, epicondyles, and a patellar surface.[6] [2] Proximally, the femur forms the hip joint, a multiaxial ball-and-socket synovial joint between the femoral head and the acetabulum of the pelvis, reinforced by ligaments such as the iliofemoral, pubofemoral, and ischiofemoral, enabling flexion, extension, abduction, adduction, and rotation while bearing significant weight.[7] [8] The acetabulum, formed by the ilium, ischium, and pubis, is deepened by the acetabular labrum, and the joint is lubricated by synovial fluid for low-friction movement.[7] Distally, the femur articulates with the tibia and patella to form the knee joint, a complex hinge-type synovial joint comprising the tibiofemoral articulations (between femoral condyles and tibial plateaus) and the patellofemoral articulation (between the patella and femoral patellar surface).[9] The patella, a sesamoid bone embedded in the quadriceps tendon, enhances leverage for knee extension and glides within the femoral trochlea.[9] This joint permits primarily flexion and extension, with limited rotation when flexed, stabilized by cruciate and collateral ligaments.[9]Musculature
The musculature of the thigh is divided into three distinct compartments by fibrous intermuscular septa attached to the femur: the anterior, medial, and posterior compartments. This organization facilitates coordinated movement and protects neurovascular structures.[10] The anterior compartment primarily contains muscles responsible for knee extension and hip flexion, innervated by the femoral nerve.[5] The posterior compartment houses the hamstrings, which extend the hip and flex the knee, supplied by the sciatic nerve.[11] The medial compartment includes the adductor muscles, which adduct the thigh, mostly innervated by the obturator nerve.[12] Anterior CompartmentThe anterior compartment consists of the sartorius and the quadriceps femoris group.[13] The sartorius, the longest muscle in the body, originates from the anterior superior iliac spine and inserts onto the medial surface of the proximal tibia via the pes anserinus; it flexes the hip and knee while externally rotating the leg.[5] The quadriceps femoris comprises four muscles: rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius.[13] Rectus femoris arises from the anterior inferior iliac spine and ilium, crossing both hip and knee joints to insert via the common quadriceps tendon into the patella and tibial tuberosity.[5] The vasti muscles originate from the femur: vastus lateralis from the lateral linea aspera and intertrochanteric line, vastus medialis from the medial linea aspera, and vastus intermedius from the anterior and lateral femoral shaft; all converge on the quadriceps tendon.[5] These muscles collectively extend the knee, with rectus femoris also contributing to hip flexion.[13] Posterior Compartment
The posterior compartment, known as the hamstrings, includes the biceps femoris, semitendinosus, and semimembranosus.[14] Biceps femoris has a long head originating from the ischial tuberosity and a short head from the linea aspera; both insert on the fibular head and lateral tibia, flexing the knee and extending the hip, with the long head also laterally rotating the leg.[11] Semitendinosus and semimembranosus arise from the ischial tuberosity; semitendinosus inserts via a long tendon to the medial tibia at the pes anserinus, while semimembranosus attaches to the medial tibial condyle and forms expansions to the meniscus and tibia.[11] Both medially rotate the leg when the knee is flexed and assist in hip extension and knee flexion.[14] The short head of biceps femoris is innervated by the common peroneal division of the sciatic nerve, distinguishing it from the other hamstrings.[11] Medial Compartment
The medial compartment contains the adductor group: pectineus, adductor longus, adductor brevis, adductor magnus, and gracilis, with obturator externus sometimes associated.[15] Pectineus originates from the pectineal line of the pubis and inserts on the pectineal line of the femur, adducting and flexing the thigh.[12] Adductor longus arises from the pubis and inserts midway along the medial femur, primarily adducting the thigh.[12] Adductor brevis, between longus and magnus, originates from the pubis and inserts proximally on the femur.[15] Adductor magnus, the largest, has pubofemoral and ischiocondylar portions from pubis/ischium to the femur and adductor tubercle, adducting and extending the thigh via its hamstring part.[12] Gracilis, a thin muscle from the pubis, inserts at the pes anserinus, adducting the thigh and flexing the knee.[15] Innervation is primarily from the obturator nerve, except adductor magnus' hamstring portion by the tibial nerve.[12]