Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Trismus
Trismus is a condition of restricted opening of the mouth. The term was initially used in the setting of tetanus. Trismus may be caused by spasm of the muscles of mastication or a variety of other causes. Temporary trismus occurs much more frequently than permanent trismus. It is known to interfere with eating, speaking, and maintaining proper oral hygiene. This interference, specifically with an inability to swallow properly, results in an increased risk of aspiration. In some instances, trismus presents with altered facial appearance. The condition may be distressing and painful. Examination and treatments requiring access to the oral cavity can be limited, or in some cases impossible, due to the nature of the condition itself.
Trismus is defined as painful restriction in opening the mouth due to a muscle spasm, however it can also refer to limited mouth opening of any cause. Another definition of trismus is simply a limitation of movement. Historically and commonly, the term lockjaw was sometimes used as a synonym for both trismus and tetanus.
Normal mouth-opening ranges from 35 to 45 mm. Males usually have slightly greater mouth opening than females. (40–60 mm, average of 50 mm). The normal lateral movement is 8–12 mm, and normal protrusive movement is approximately 10 mm.[medical citation needed] Some have distinguished mild trismus as 20–30 mm interincisal opening, moderate as 10–20 mm and severe as less than 10 mm.
Trismus is derived from the Greek word trigmos/trismos meaning "a scream; a grinding, rasping or gnashing".
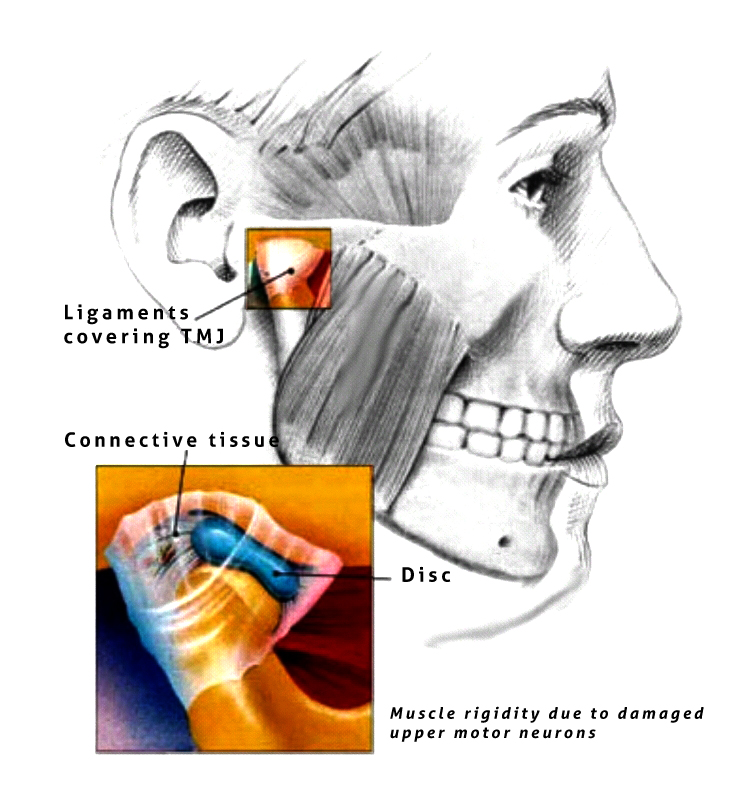
Traditionally causes of trismus are divided into intra-articular (factors within the temporomandibular joint [TMJ]) and extra-articular (factors outside the joint, see table).
Fractures, particularly those of the mandible and fractures of zygomatic arch and zygomatic arch complex, accidental incorporation of foreign bodies due to external traumatic injury. Treatment: fracture reduction, removal of foreign bodies with antibiotic coverage[citation needed]
Rarely, trismus is a symptom of nasopharyngeal or infratemporal tumors/ fibrosis of temporalis tendon, when patient has limited mouth opening, always premalignant conditions like oral submucous fibrosis (OSMF) should also be considered in differential diagnosis.
Succinyl choline, phenothiazines and tricyclic antidepressants causes trismus as a secondary effect. Trismus can be seen as an extra-pyramidal side-effect of metoclopromide, phenothiazines and other medications.
Hub AI
Trismus AI simulator
(@Trismus_simulator)
Trismus
Trismus is a condition of restricted opening of the mouth. The term was initially used in the setting of tetanus. Trismus may be caused by spasm of the muscles of mastication or a variety of other causes. Temporary trismus occurs much more frequently than permanent trismus. It is known to interfere with eating, speaking, and maintaining proper oral hygiene. This interference, specifically with an inability to swallow properly, results in an increased risk of aspiration. In some instances, trismus presents with altered facial appearance. The condition may be distressing and painful. Examination and treatments requiring access to the oral cavity can be limited, or in some cases impossible, due to the nature of the condition itself.
Trismus is defined as painful restriction in opening the mouth due to a muscle spasm, however it can also refer to limited mouth opening of any cause. Another definition of trismus is simply a limitation of movement. Historically and commonly, the term lockjaw was sometimes used as a synonym for both trismus and tetanus.
Normal mouth-opening ranges from 35 to 45 mm. Males usually have slightly greater mouth opening than females. (40–60 mm, average of 50 mm). The normal lateral movement is 8–12 mm, and normal protrusive movement is approximately 10 mm.[medical citation needed] Some have distinguished mild trismus as 20–30 mm interincisal opening, moderate as 10–20 mm and severe as less than 10 mm.
Trismus is derived from the Greek word trigmos/trismos meaning "a scream; a grinding, rasping or gnashing".
Traditionally causes of trismus are divided into intra-articular (factors within the temporomandibular joint [TMJ]) and extra-articular (factors outside the joint, see table).
Fractures, particularly those of the mandible and fractures of zygomatic arch and zygomatic arch complex, accidental incorporation of foreign bodies due to external traumatic injury. Treatment: fracture reduction, removal of foreign bodies with antibiotic coverage[citation needed]
Rarely, trismus is a symptom of nasopharyngeal or infratemporal tumors/ fibrosis of temporalis tendon, when patient has limited mouth opening, always premalignant conditions like oral submucous fibrosis (OSMF) should also be considered in differential diagnosis.
Succinyl choline, phenothiazines and tricyclic antidepressants causes trismus as a secondary effect. Trismus can be seen as an extra-pyramidal side-effect of metoclopromide, phenothiazines and other medications.