Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Lymphatic system
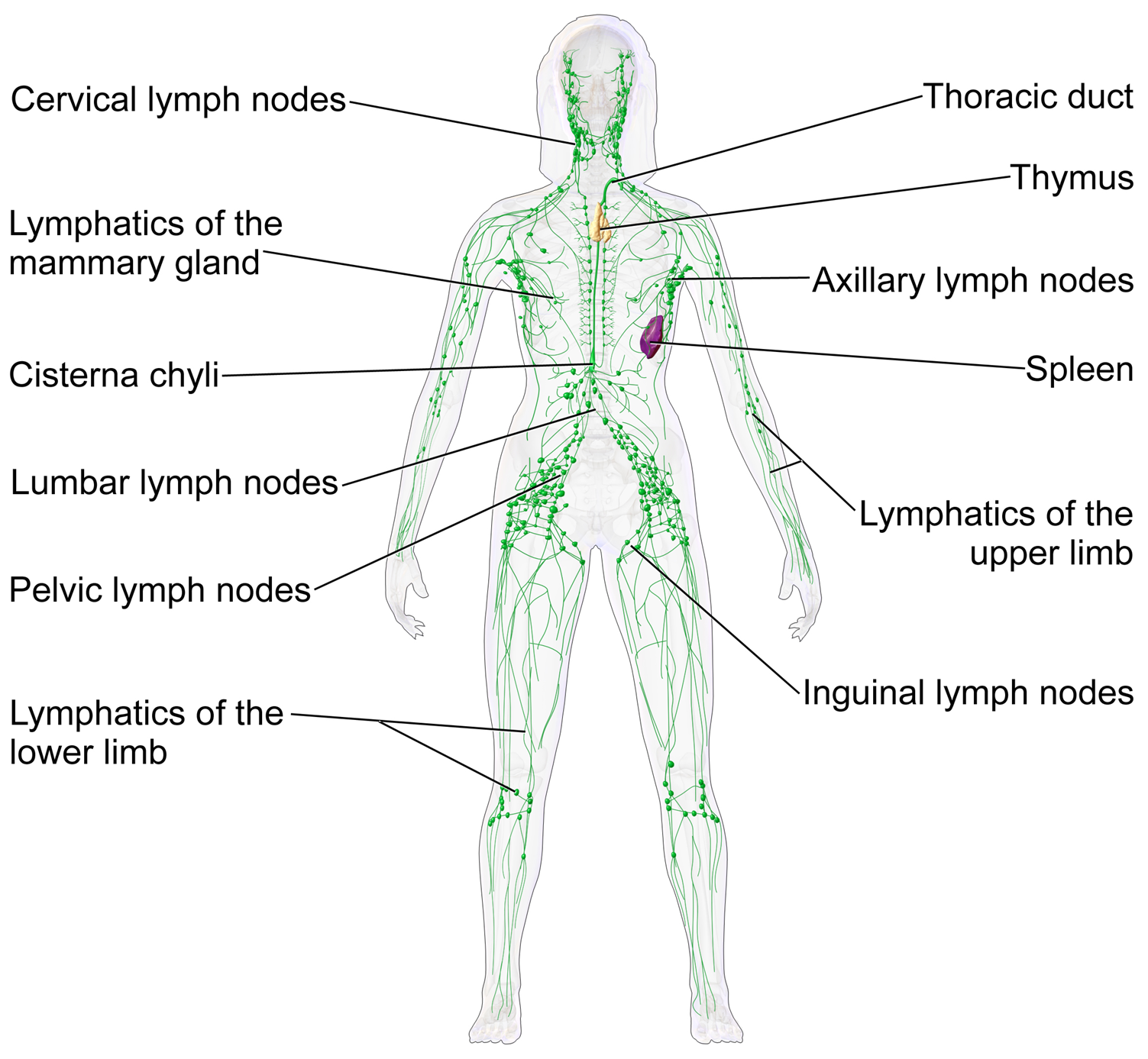
The lymphatic system, or lymphoid system, is an organ system in vertebrates that is part of the immune system and complementary to the circulatory system. It consists of a large network of lymphatic vessels, lymph nodes, lymphoid organs, lymphatic tissue and lymph. The Latin word for lymph, lympha, refers to the deity of fresh water, "Lympha".
Unlike the circulatory system, which is a closed system, the lymphatic system is open. Lymph originates in the interstitial fluid that leaks from blood in the circulatory system into the tissues of the body. This fluid carries nutrients to the cells and collects waste products, bacteria, and damaged cells, before draining into the lymphatic vessels as lymph. The circulatory system processes an average of 20 litres (5.3 US gal) of blood per day through capillary filtration, which removes plasma from the blood. Roughly 17 litres (4.5 US gal) of the filtered blood is reabsorbed directly into the blood vessels, while the remaining 3 litres (0.79 US gal) are left in the interstitial fluid. The lymphatic system provides an accessory return route to the blood for this remainder.
The other main function is that of immune defense. Lymph is very similar to blood plasma, in that it contains waste products and cellular debris, together with bacteria and proteins. The cells of the lymph are mostly lymphocytes. Associated lymphoid organs are composed of lymphoid tissue, and are the sites either of lymphocyte production or of lymphocyte activation. These include the lymph nodes (where the highest lymphocyte concentration is found), the spleen, the thymus, and the tonsils. Lymphocytes are initially generated in the bone marrow. The lymphoid organs also contain other types of cells such as stromal cells for support. Lymphoid tissue is also associated with mucosas such as mucosa-associated lymphoid tissue (MALT).
These vessels carry the lymph throughout the body, passing through numerous lymph nodes which filter out unwanted materials such as bacteria and damaged cells. Lymph then passes into much larger lymph vessels known as lymph ducts. The right lymphatic duct drains the right side of the region and the much larger left lymphatic duct, known as the thoracic duct, drains the left side of the body. The ducts empty into the subclavian veins to return to the blood circulation. Lymph is moved through the system by muscle contractions. In some vertebrates, a lymph heart is present that pumps the lymph to the veins.
The lymphatic system was first described in the 17th century independently by Olaus Rudbeck and Thomas Bartholin.
The lymphatic system consists of a conducting network of lymphatic vessels, lymphoid organs, lymphoid tissues, and the circulating lymph.
The primary (or central) lymphoid organs, including the thymus, bone marrow, fetal liver and yolk sac, are responsible for generating lymphocytes from immature progenitor cells in the absence of antigens. The thymus and the bone marrow constitute the primary lymphoid organs involved in the production and early clonal selection of lymphocyte tissues.
Bird species' primary lymphoid organs include the bone marrow, thymus, bursa of Fabricius, and yolk sac.
Hub AI
Lymphatic system AI simulator
(@Lymphatic system_simulator)
Lymphatic system
The lymphatic system, or lymphoid system, is an organ system in vertebrates that is part of the immune system and complementary to the circulatory system. It consists of a large network of lymphatic vessels, lymph nodes, lymphoid organs, lymphatic tissue and lymph. The Latin word for lymph, lympha, refers to the deity of fresh water, "Lympha".
Unlike the circulatory system, which is a closed system, the lymphatic system is open. Lymph originates in the interstitial fluid that leaks from blood in the circulatory system into the tissues of the body. This fluid carries nutrients to the cells and collects waste products, bacteria, and damaged cells, before draining into the lymphatic vessels as lymph. The circulatory system processes an average of 20 litres (5.3 US gal) of blood per day through capillary filtration, which removes plasma from the blood. Roughly 17 litres (4.5 US gal) of the filtered blood is reabsorbed directly into the blood vessels, while the remaining 3 litres (0.79 US gal) are left in the interstitial fluid. The lymphatic system provides an accessory return route to the blood for this remainder.
The other main function is that of immune defense. Lymph is very similar to blood plasma, in that it contains waste products and cellular debris, together with bacteria and proteins. The cells of the lymph are mostly lymphocytes. Associated lymphoid organs are composed of lymphoid tissue, and are the sites either of lymphocyte production or of lymphocyte activation. These include the lymph nodes (where the highest lymphocyte concentration is found), the spleen, the thymus, and the tonsils. Lymphocytes are initially generated in the bone marrow. The lymphoid organs also contain other types of cells such as stromal cells for support. Lymphoid tissue is also associated with mucosas such as mucosa-associated lymphoid tissue (MALT).
These vessels carry the lymph throughout the body, passing through numerous lymph nodes which filter out unwanted materials such as bacteria and damaged cells. Lymph then passes into much larger lymph vessels known as lymph ducts. The right lymphatic duct drains the right side of the region and the much larger left lymphatic duct, known as the thoracic duct, drains the left side of the body. The ducts empty into the subclavian veins to return to the blood circulation. Lymph is moved through the system by muscle contractions. In some vertebrates, a lymph heart is present that pumps the lymph to the veins.
The lymphatic system was first described in the 17th century independently by Olaus Rudbeck and Thomas Bartholin.
The lymphatic system consists of a conducting network of lymphatic vessels, lymphoid organs, lymphoid tissues, and the circulating lymph.
The primary (or central) lymphoid organs, including the thymus, bone marrow, fetal liver and yolk sac, are responsible for generating lymphocytes from immature progenitor cells in the absence of antigens. The thymus and the bone marrow constitute the primary lymphoid organs involved in the production and early clonal selection of lymphocyte tissues.
Bird species' primary lymphoid organs include the bone marrow, thymus, bursa of Fabricius, and yolk sac.