
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Addiction AI simulator
(@Addiction_simulator)
Hub AI
Addiction AI simulator
(@Addiction_simulator)
Addiction
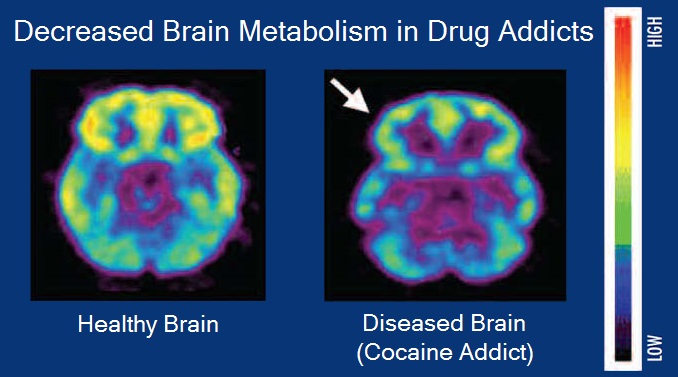
Addiction is a neuropsychological disorder characterized by a persistent and intense urge to use a drug or engage in a behavior that produces natural reward, despite substantial harm and other negative consequences. Repetitive drug use can alter brain function in synapses similar to natural rewards like food or falling in love in ways that perpetuate craving and weakens self-control for people with pre-existing vulnerabilities. This phenomenon – drugs reshaping brain function – has led to an understanding of addiction as a brain disorder with a complex variety of psychosocial as well as neurobiological factors that are implicated in the development of addiction. While mice given cocaine showed the compulsive and involuntary nature of addiction, for humans this is more complex, related to behavior or personality traits.
Classic signs of addiction include compulsive engagement in rewarding stimuli, preoccupation with substances or behavior, and continued use despite negative consequences. Habits and patterns associated with addiction are typically characterized by immediate gratification (short-term reward), coupled with delayed deleterious effects (long-term costs).
Examples of substance addiction include alcoholism, cannabis addiction, amphetamine addiction, cocaine addiction, nicotine addiction, opioid addiction, and eating or food addiction. Behavioral addictions may include gambling addiction, shopping addiction, stalking, pornography addiction, internet addiction, social media addiction, video game addiction, and sexual addiction. The DSM-5 and ICD-10 only recognize gambling addictions as behavioral addictions, but the ICD-11 also recognizes gaming addictions.
Signs and symptoms of drug addiction can vary depending on the type of addiction. Symptoms may include:
Other signs and symptoms can be categorized across relevant dimensions:
The DSM-5 discourages using the term "drug addiction" because of its "uncertain definition and its potentially negative connotation" and prefers the term "substance use disorder" to describe the wide range of the disorder, from a mild form to a severe state of chronically relapsing, compulsive pattern of drug taking.
SUD, belongs to the class of substance-related disorders, is a chronic and relapsing brain disorder that features drug seeking and drug abuse, despite their harmful effects. This form of addiction changes brain circuitry such that the brain's reward system is compromised, causing functional consequences for stress management and self-control. Damage to the functions of the organs involved can persist throughout a lifetime and cause death if untreated. Substances involved with drug addiction include alcohol, nicotine, marijuana, opioids, cocaine, amphetamines, and even foods with high fat and sugar content. Addictions can begin experimentally in social contexts and can arise from the use of prescribed medications or a variety of other measures.
It has been shown to work in phenomenological, conditioning (operant and classical), cognitive models, and the cue reactivity model. However, no one model completely illustrates substance abuse.
Addiction
Addiction is a neuropsychological disorder characterized by a persistent and intense urge to use a drug or engage in a behavior that produces natural reward, despite substantial harm and other negative consequences. Repetitive drug use can alter brain function in synapses similar to natural rewards like food or falling in love in ways that perpetuate craving and weakens self-control for people with pre-existing vulnerabilities. This phenomenon – drugs reshaping brain function – has led to an understanding of addiction as a brain disorder with a complex variety of psychosocial as well as neurobiological factors that are implicated in the development of addiction. While mice given cocaine showed the compulsive and involuntary nature of addiction, for humans this is more complex, related to behavior or personality traits.
Classic signs of addiction include compulsive engagement in rewarding stimuli, preoccupation with substances or behavior, and continued use despite negative consequences. Habits and patterns associated with addiction are typically characterized by immediate gratification (short-term reward), coupled with delayed deleterious effects (long-term costs).
Examples of substance addiction include alcoholism, cannabis addiction, amphetamine addiction, cocaine addiction, nicotine addiction, opioid addiction, and eating or food addiction. Behavioral addictions may include gambling addiction, shopping addiction, stalking, pornography addiction, internet addiction, social media addiction, video game addiction, and sexual addiction. The DSM-5 and ICD-10 only recognize gambling addictions as behavioral addictions, but the ICD-11 also recognizes gaming addictions.
Signs and symptoms of drug addiction can vary depending on the type of addiction. Symptoms may include:
Other signs and symptoms can be categorized across relevant dimensions:
The DSM-5 discourages using the term "drug addiction" because of its "uncertain definition and its potentially negative connotation" and prefers the term "substance use disorder" to describe the wide range of the disorder, from a mild form to a severe state of chronically relapsing, compulsive pattern of drug taking.
SUD, belongs to the class of substance-related disorders, is a chronic and relapsing brain disorder that features drug seeking and drug abuse, despite their harmful effects. This form of addiction changes brain circuitry such that the brain's reward system is compromised, causing functional consequences for stress management and self-control. Damage to the functions of the organs involved can persist throughout a lifetime and cause death if untreated. Substances involved with drug addiction include alcohol, nicotine, marijuana, opioids, cocaine, amphetamines, and even foods with high fat and sugar content. Addictions can begin experimentally in social contexts and can arise from the use of prescribed medications or a variety of other measures.
It has been shown to work in phenomenological, conditioning (operant and classical), cognitive models, and the cue reactivity model. However, no one model completely illustrates substance abuse.
Recent media
Recent media